Verrucous Carcinoma (and Variants)
Elsa F. Velazquez, MD
Key Facts
Clinical Issues
Unicentric tumors are more frequent but multicentric ones may occur
Some cases may be associated with viral warts (plantar lesions)
VC may arise in the setting of longstanding lichen sclerosus (genital tumors)
Macroscopic Features
Exophytic papillary tumor
Broad and pushing base
Deep burrowing pattern is hallmark of carcinoma cuniculatum (VC variant)
Microscopic Pathology
Acanthotic papillae
Slender fibrovascular cores
Prominent (orange) keratin craters between papillae
Lack of koilocytosis
Extremely well differentiated
Epithelium of papillae and keratin predominate over fibrovascular core
Pushing, club-shaped base
Higher grade areas &/or infiltrative borders are not features of pure VC and raise possibility of hybrid (mixed) VC
Top Differential Diagnoses
Carcinoma cuniculatum (VC variant)
Mixed/hybrid VC with foci of SCC of usual type
Condyloma acuminatum/giant condyloma
Warty (condylomatous) carcinoma
Papillary carcinoma (SCC variant)
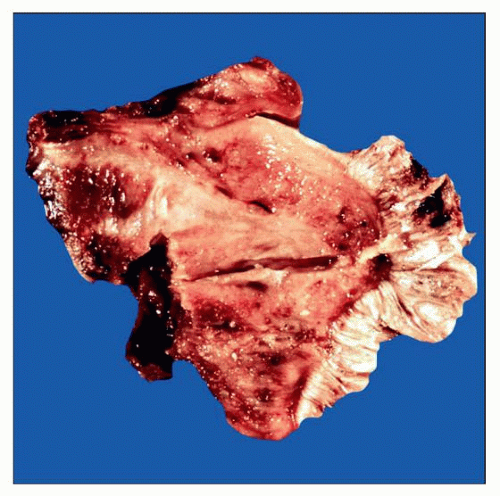 Cut section of a partial penectomy specimen shows a verruciform tumor with sharp bulbous base confined to the lamina propria. Note the papillomatous and spiky surface. |
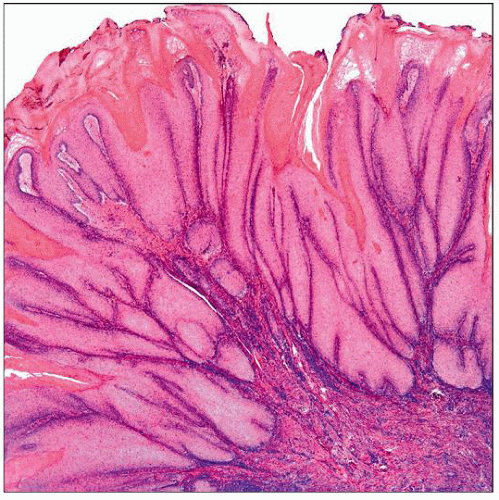 Low-power view of a verrucous carcinoma illustrates the thick acanthotic papillae, thin fibrovascular cores, and the classic piling up of keratin between papillae. |
TERMINOLOGY
Abbreviations
Verrucous carcinoma (VC), squamous cell carcinoma (SCC)
Synonyms
Buschke-Loewenstein tumor
Ackerman tumor (oral florid papillomatosis)
Definitions
Very well-differentiated verruciform SCC with bulbous deep borders and lack of koilocytosis
ETIOLOGY/PATHOGENESIS
Unknown Pathogenesis
Cutaneous (particularly plantar) lesions may be associated with HPV and arise within preexisting warts
Cutaneous lesions may be related to scarring and chronic inflammation
Oral VC (Ackerman tumor) may be related to tobacco chewing
Anogenital cases may be associated with phimosis and lichen sclerosus
Anogenital VC are associated with HPV6 in some cases
CLINICAL ISSUES
Epidemiology
Incidence
Rare
Age
6th-7th decade
Site
Originally described by Lauren Ackerman in the oral cavity
May also affect anogenital area and skin (sole of the foot, finger, nail bed, scalp, wrist, buttocks, etc.)
Presentation
Exophytic white-gray neoplasm
Unicentric tumors are more frequent than multicentric ones
Treatment
Surgical
Prognosis
Pure VCs have excellent prognosis
Tumors may recur but almost never metastasize
Hybrid/mixed VCs have worse prognosis than pure VC
Sporadic reports of sarcomatoid/anaplastic transformation after radiation therapy
MACROSCOPIC FEATURES
General Features
Exophytic white-gray neoplasms with papillary, sometimes spiky surface
Cut sections reveal broad base between tumor and stroma
Tumors may invade deep dermis and deeper structures
Irregular jagged borders or foci of necrosis are not features of pure verrucous carcinoma
Size
1-3 cm in diameter
MICROSCOPIC PATHOLOGY
Histologic Features
Extremely well-differentiated squamous neoplasm
Thick acanthotic papillae with slender fibrovascular cores
Papillae are separated by prominent keratin craters
Orthokeratosis with presence of granular layer
Parakeratosis may be occasional
Absence of koilocytosis
Pushing, club-shaped deep borders
Adjacent epithelium often shows verrucous squamous hyperplasia &/or differentiated vulvar or penile intraepithelial neoplasia (differentiated VIN or PeIN)
Some cases associated with background of lichen sclerosus (genital)
Predominant Pattern/Injury Type



