Venous Access: The Subclavian Vein and the Cephalic Vein in the Deltopectoral Groove
Percutaneous cannulation of the subclavian vein is frequently used for rapid access to the central venous circulation and for the placement of long-term intravascular access devices such as tunneled catheters and ports. Because the vein follows a relatively constant course that is easily estimated by readily palpable bony landmarks, this is a convenient site for cannulation. However, this vein’s proximity to other major vascular structures and to the apex of the lung necessitates a thorough understanding of the anatomy so that complications may be avoided when performing this routine procedure. Two approaches to this procedure are described—first, cannulation by anatomic landmarks; second, cannulation under ultrasound guidance. Details on the Seldinger technique are illustrated and described in Chapter 8 (Figure 8.6) and will not be repeated here.
Performing a cutdown on the cephalic vein in the deltopectoral groove is an alternative mean of achieving access to the central circulation. In selected patients, it may be easier or safer than percutaneous methods.
The subclavian and deltopectoral groove approaches may also be used for the placement of implantable venous access devices. Details on these devices and how to place them are included in Chapter 8 (Figures 8.9 and 8.10) and are not repeated here.
SCORE™, the Surgical Council on Resident Education, classified Central venous line placement, Ultrasound use for intravascular access, and Insertion of implantable venous access devices as “ESSENTIAL COMMON” procedures.
LIST OF STRUCTURES
Superior vena cava
Brachiocephalic (Innominate) Vein
Internal jugular vein
Subclavian vein
Vertebral vein
Inferior thyroid vein
Internal thoracic vein
Thymic vein
Left superior intercostal vein
Axillary vein
Cephalic vein
Aorta
Brachiocephalic artery
Subclavian artery
Thoracic Duct
Arch of thoracic duct
Cervical portion of thoracic duct
Thoracic portion of thoracic duct
Acromion process
Sternal notch
Clavicle
Sternoclavicular joints
Anterior scalene muscle
Sternohyoid muscle
Sternothyroid muscle
Pectoralis major muscle
Pectoralis minor muscle
Clavipectoral fascia
Prevertebral fascia
Deltopectoral groove
Deltopectoral triangle
Pleura
Thymus
Trachea
Phrenic nerve
Vagus nerve
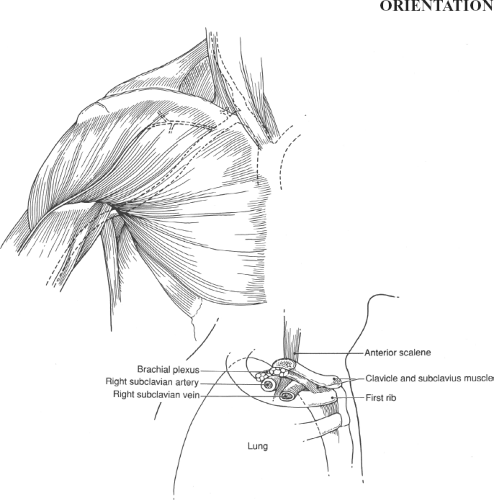 Figure 14.1 Regional anatomy. Note that the subclavian vein passes anterior to the subclavian artery and anterior scalene muscle. |
Percutaneous Cannulation of the Subclavian Vein by Landmarks
Cannulation by Landmarks—Positioning the Patient and Identifying Landmarks (Fig. 14.2)
Technical Points
Position the patient supine with arms at the side. Elevate the foot of the bed to a 5- or 10-degree Trendelenburg position. This will increase venous pressure in the central veins, distending the subclavian vein and rendering the possibility of venous air embolus less likely. Place a vertical roll under the thoracic spine to allow the shoulders to “fall back” slightly, thus opening the angle between the clavicle and the ribs. Inspect both infraclavicular regions for evidence of previous cannulation or local infections. In general, the left subclavian vein is somewhat easier to cannulate and will more reliably provide access to the central circulation than the right subclavian vein. Both, however, are usable.
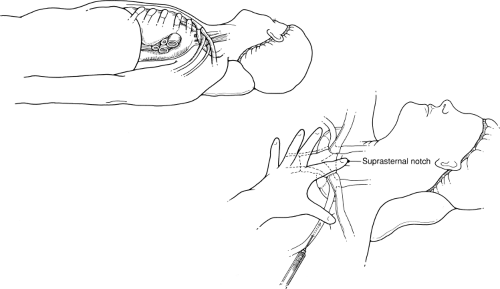 Figure 14.2 Positioning the patient and identifying landmarks—subclavian venous cannulation by landmarks |
STEPS IN PROCEDURE—PERCUTANEOUS SUBCLAVIAN VENOUS CANNULATION
Position patient with ipsilateral arm at side and in slight Trendelenburg position
Place a roll under the thoracic spine to open up the infraclavicular space, if necessary
Identify the following bony landmarks: Acromion process, sternal notch, and medial third of the clavicle
Place Index Finger of Nondominant Hand in Sternal Notch and Hook the Thumb Under the Clavicle
Usually one-third of the distance from the acromion to the sternal notch
Infiltrate skin and subcutaneous tissues
Maintaining needle parallel to plane of floor, walk the needle under the clavicle and aspirate to find the vein
Pass larger needle supplied with the kit into the vein; confirm free flow of venous blood
Pass guidewire under fluoroscopic guidance
Make skin incision
Pass dilator and sheath
Pass catheter through sheath, peel away sheath and remove
Confirm catheter position
Secure catheter
HALLMARK ANATOMIC COMPLICATIONS—PERCUTANEOUS SUBCLAVIAN CANNULATION
Pneumothorax
Subclavian artery cannulation
Mediastinal perforation
Catheter placed too far medial; pinched off by clavicle
Identify the constant bony landmarks before cannulation. These include the acromion process, the sternal notch, and the medial third of the clavicle. Prepare and drape a field that includes the medial half of the clavicle. Using your nondominant hand, place the index finger in the sternal notch and the thumb under the clavicle. Identify the place where the curvature of the clavicle begins to change (remember that the clavicle is S-shaped). This should be about one-third of the distance from the sternal notch to the acromion and medial to the pulse of the subclavian artery if it is palpable. Use a fine-gauge needle to infiltrate the area with lidocaine without epinephrine. Aspirate as the skin, subcutaneous tissues, and periosteum are infiltrated. “Walk” the needle under the periosteum of the clavicle and aspirate. Free aspiration of venous blood with this fine-gauge
needle will help to identify where the subclavian vein lies. Do not inject local anesthesia into the subclavian vein.
needle will help to identify where the subclavian vein lies. Do not inject local anesthesia into the subclavian vein.
After identifying the probable location of the subclavian vein, place an 18-gauge needle on a Luer slip syringe. Maintaining the orientation of the bony landmarks previously described, “walk” the tip of the needle under the clavicle. The point of the needle should be aimed at the sternal notch. The shaft of the needle should remain parallel to the floor at all times. Never point the needle toward the chest wall. You should feel the needle strike the periosteum of the underside of the clavicle and slip under the clavicle; aspirate until free return of venous blood is obtained.
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


