Transsacral Approach to Rectal Lesions
The transsacral approach is most commonly used for resection of benign retrorectal tumors or for removal of sessile polyps that cannot be reached by other approaches to the rectum. It is a useful approach to the retrorectal space. It has also been described as a means of access for low anastomosis, but use of the circular stapling device has largely superseded this approach.
Steps in Procedure
Approach for Large Tumors
Patient in right lateral decubitus position with abdomen and sacrum draped
Enter presacral space through the abdomen
Gain vascular control
Mobilize tumor from presacral space and rectum
Pack wound and turn attention to sacral region
Transverse incision 10 cm long over sacrococcygeal joint
Deepen incision to periosteum of bone
Divide joint with heavy scissors and resect coccyx
Enter retrorectal space
Resect part of sacrum up to the third segment if necessary with tumor
Remove entire tumor
Posterior Approach for Small Tumors
Prone jackknife position
Transverse incision over sacrococcygeal joint
Divide joint and enter retrorectal space as noted above
Separate tumor from underlying rectal wall
Tumor must be completely resected
Hallmark Anatomic Complications
Bleeding from presacral venous plexus
Injury to rectum
Sacral nerve dysfunction
List of Structures
Sacrum
Coccyx
Sacrococcygeal joint
Presacral fascia
Piriformis muscle
Iliacus muscle
Coccygeus muscle
Multifidus muscles
Gluteus maximus muscle
Levator ani muscle
Anococcygeal ligament
Presacral venous plexus
Rectum
Anal canal
Internal anal sphincter
External anal sphincter
Intersphincteric groove
Pectinate line
Puborectalis muscle
Inferior Mesenteric Artery
Superior rectal (hemorrhoidal) artery
Common Iliac artery and Vein
Internal iliac artery and vein
Middle rectal (hemorrhoidal) artery and vein
Internal pudendal artery and vein
External iliac artery and vein
Inferior rectal (hemorrhoidal) artery and vein
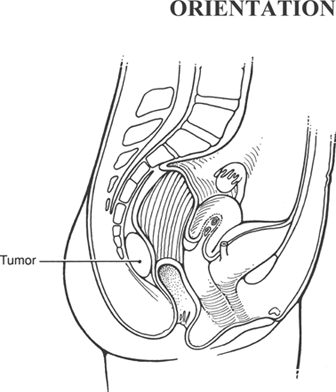 |
Incision and Exposure of the Retrorectal Space (Fig. 101.1)
Technical Points
A combined abdominal and transsacral approach is recommended for removal of large retrorectal tumors. In this case, the patient should be prepped with both the abdominal and sacral regions exposed. The retrorectal or presacral area is approached transabdominally by the same approach that is used for abdominoperineal resection (see Chapter 83). The sacral portion of the operation is described here. Small tumors may be approached transsacrally, without entering the abdomen. The combined approach provides adequate exposure for complete and adequate excision. This is especially important with tumors that extend up into the pelvis, and this approach allows excellent hemostatic control.
Place the patient in the right lateral decubitus position. Make a transverse incision, about 10 cm in length, over the sacrococcygeal joint. Confirm the position of the sacrococcygeal joint by palpation with an index finger within the anal canal if necessary. Deepen this incision until the periosteum of the bone is encountered. Divide the sacrococcygeal joint with heavy scissors. The coccyx may be removed with the specimen. Enter the retrorectal space by sharp and blunt dissection. It will be necessary to divide the periosteum and ligamentous attachments at the sacrococcygeal joint to do this. The next large structure that will be encountered is the muscular wall of the rectum, which can easily be surrounded and dissected free. Many tumors are attached to the coccyx or lower segments of the sacrum. Up to the third segment of the sacrum may be removed at the time of tumor resection without functional impairment. Removal of the sacral nerve roots up to S1 or S2 has been relatively well tolerated and is preferable to tumor recurrence.
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


