Total Abdominal Hysterectomy and Salpingo-Oophorectomy
Hysterectomy may be performed transabdominally or vaginally. One or both ovaries may be removed with the uterus. In this chapter, total abdominal hysterectomy with bilateral salpingo-oophorectomy is described. Modification of the technique to preserve one or both ovaries is also discussed. References at the end of the chapter describe supracervical and transvaginal hysterectomy. Chapter 104 provides an introduction to laparoscopic surgery of the female pelvis.
SCORE™, the Surgical Council on Resident Education, classified hysterectomy and salpingo-oophorectomy as “ESSENTIAL UNCOMMON” procedures.
STEPS IN PROCEDURE
Lithotomy position; empty bladder with catheter
Skin crease transverse incision
Raise flap cephalad and make vertical midline incision through fascia
Thorough abdominal exploration
Grasp uterine fundus with two Kelly clamps and elevate
Divide round ligaments with clamps and ties
If ovary is to be spared, divide uterine tube and ovarian ligament
If ovary is to be taken, incise broad ligament lateral to tube and ovary
Identify and protect ureter
Secure uterine vessels
Incise peritoneum overlying bladder and create bladder flap
Continue dissection to uterine cervix and divide
Vaginal cuff may be closed with running lock stitch or oversewn and left open
Close abdomen in usual fashion without drains
HALLMARK ANATOMIC COMPLICATIONS
Injury to ureter
Injury to bladder
LIST OF STRUCTURES
Uterus
Cervix
Vagina
Fallopian (uterine) tubes
Ovaries
Round ligament
Broad ligament
Suspensory (infundibulopelvic) ligament
Ovarian ligament
Lateral cervical (cardinal) ligament
Uterosacral ligament
Bladder
Ureter
Urachus
Vesicouterine pouch (anterior cul-de-sac)
Rectouterine pouch (posterior cul-de-sac, pouch of Douglas)
Rectovaginal fascia
Internal iliac artery
Uterine Artery
Tubal branch
Ovarian branch
Ovarian artery
Rectus abdominis muscle
Anterior rectus sheath
Linea alba
Pyramidalis muscle
Transversalis fascia
Incision and Initial Exposure (Fig. 103.1)
Technical Points
Place the patient in the lithotomy position. Empty the bladder by straight catheterization or by placing an indwelling Foley catheter. After general anesthesia has been administered, perform a pelvic examination to confirm the anatomy. A Trendelenburg position of about 15 degrees will facilitate pelvic exposure.
Total abdominal hysterectomy may be performed through a lower midline incision. However, the more cosmetically appealing Pfannenstiel incision is described here.
Make a transverse incision in the natural skin crease where the skin incision will be hidden by regrowth of pubic hair. Make the incision about 10 to 15 cm long, depending on the habitus of the patient. Carry this incision through skin and subcutaneous tissue to the underlying rectus sheath. Incise the anterior rectus sheath in line with the skin incision. Develop flaps between the anterior rectus sheath and the underlying rectus muscle until the muscle is exposed well in the midline to about the level of the umbilicus. Retract the rectus muscles laterally to expose the midline fascia and underlying peritoneum. Incise the fascia and peritoneum vertically from the umbilicus to the pubis. Identify the bladder in the inferior aspect of the incision and gently retract it downward, out of harm’s way. Exposure through this incision is quite limited. Use it only when you do not anticipate a need for access to the upper abdomen.
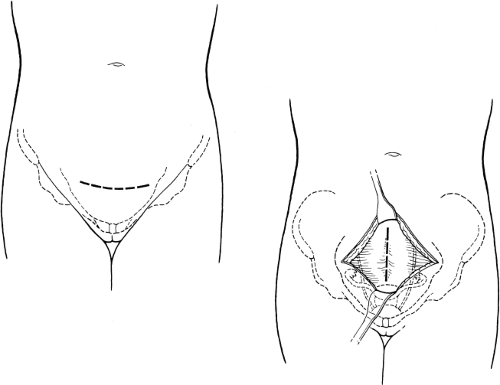 Figure 103.1 Incision and initial exposure |
Anatomic Points
The infraumbilical vertical midline incision exposes a very narrow linea alba, from which fibers of the rectus abdominis muscle originate and upon which the more anterior pyramidalis muscle inserts; this makes a true midline incision technically difficult. If the exact midline is not divided, then this becomes a muscle-splitting incision through the pyramidalis and rectus abdominis muscles. Surgically, the posterior rectus sheath ends approximately halfway between the umbilicus and the pubis, at the arcuate line. Inferior to this line, the posterior surface of the rectus abdominis muscle is in contact with the transversalis fascia.
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


