|
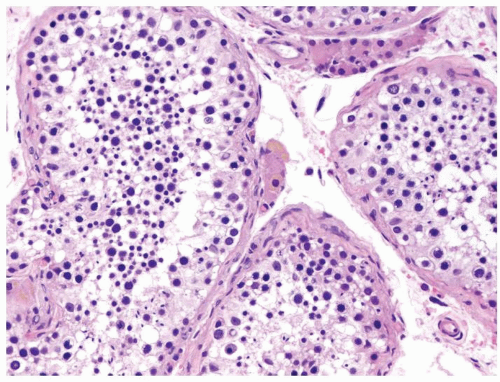 Figure 4.1.1 Normal adult seminiferous tubules showing normal spermatogenesis from spermatogonia to spermatozoa. Note the presence of primary and secondary spermatocytes and spermatids in variable proportions. |
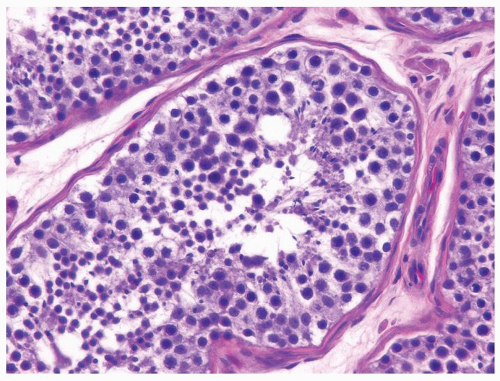 Figure 4.1.2 Normal adult seminiferous tubules showing normal spermatogenesis. |
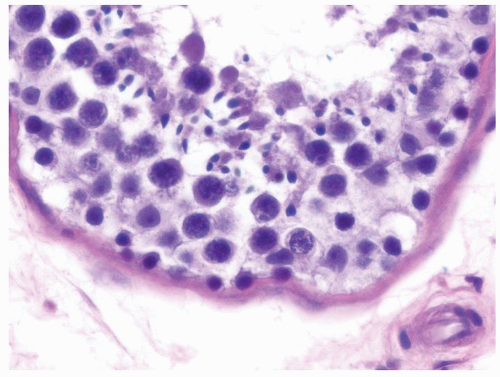 Figure 4.1.3 Normal adult seminiferous tubules showing normal spermatogenesis. |
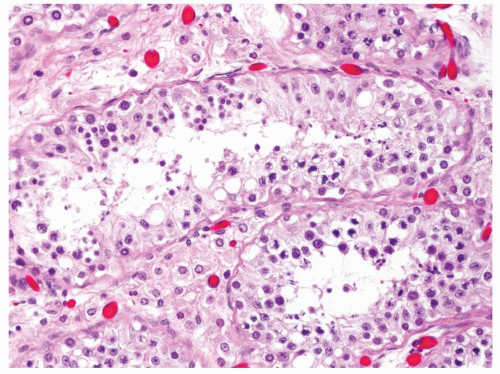 Figure 4.1.4 Adult seminiferous tubules with hypospermatogenesis. The overall total number of germ cells is decreased. |
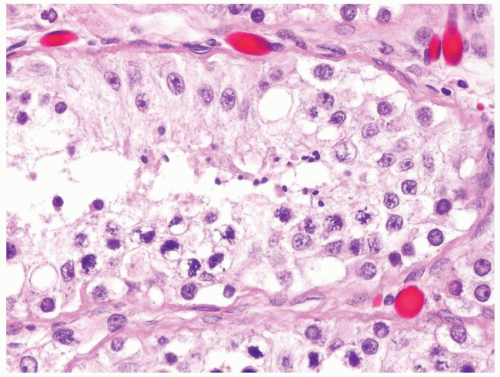 Figure 4.1.5 Adult seminiferous tubules with hypospermatogenesis. |
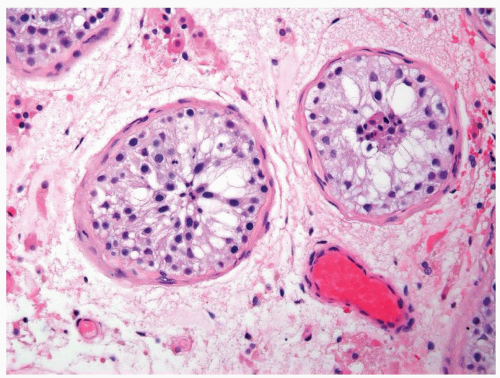 Figure 4.1.6 Adult seminiferous tubules with marked hypospermatogenesis. |
|
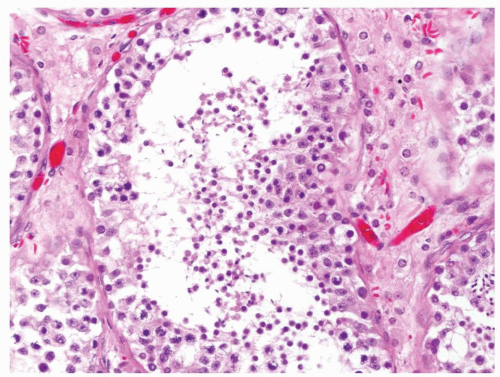 Figure 4.2.1 Adult seminiferous tubules with hypospermatogenesis. Full maturation through all spermatogenic stages occur, but the overall total number of germ cells is decreased. |
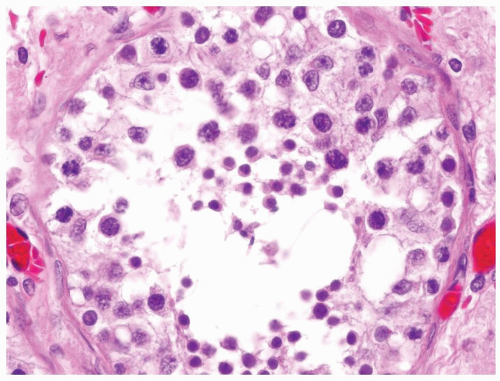 Figure 4.2.2 Adult seminiferous tubules with hypospermatogenesis. |
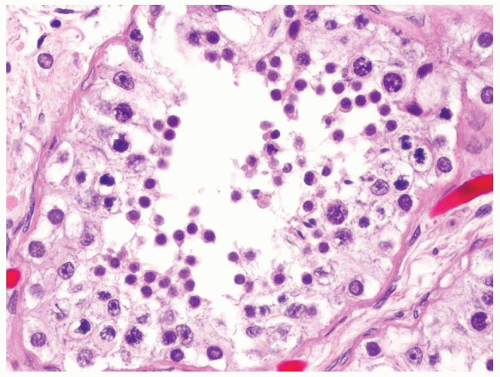 Figure 4.2.3 Adult seminiferous tubules with hypospermatogenesis. |
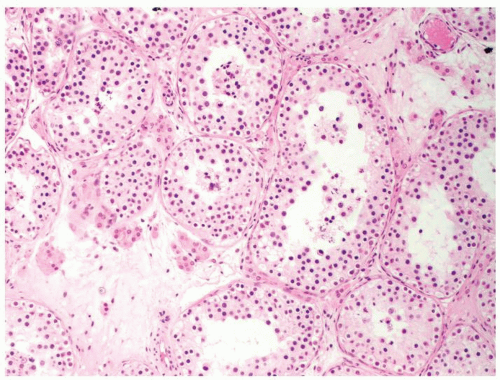 Figure 4.2.4 Adult seminiferous tubules showing maturation arrest at the secondary spermatocyte phase. Note absence of spermatid and spermatozoa. |
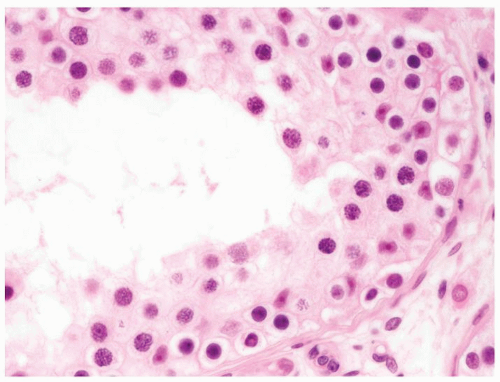 Figure 4.2.5 Adult seminiferous tubules showing maturation arrest at the secondary spermatocyte phase. |
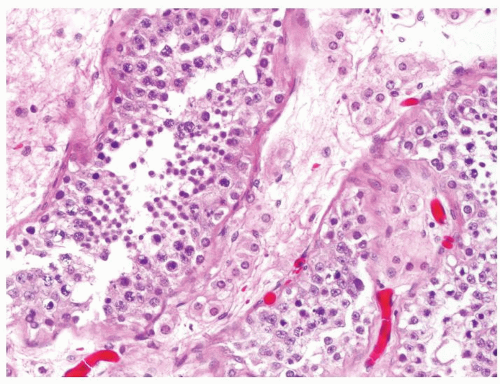 Figure 4.2.6 Adult seminiferous tubules showing maturation arrest at the spermatid phase. |
|
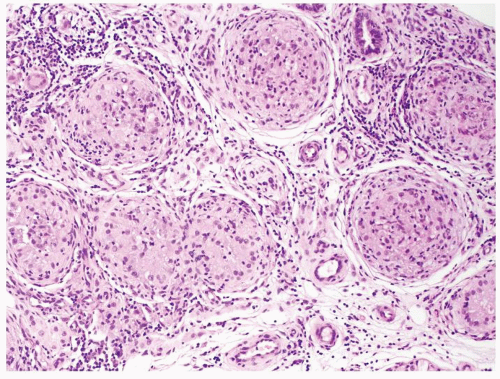 Figure 4.3.1 Idiopathic granulomatous orchitis showing nonnecrotizing granulomas filling seminiferous tubules. Granulomas are composed of epithelioid histiocytes, giant cells admixed with lymphocytes and plasma cells. |
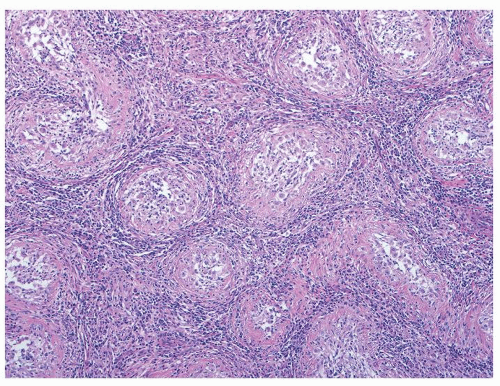 Figure 4.3.2 Idiopathic granulomatous orchitis. Granulomas are composed of epithelioid histiocytes and giant cells. |
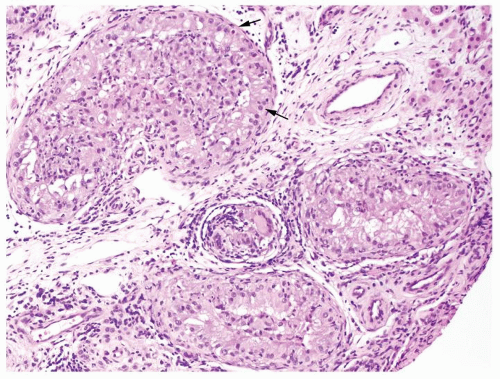 Figure 4.3.3 Idiopathic granulomatous orchitis showing nonnecrotizing granulomas filling seminiferous tubules. Residual germ cells are noted (arrows). |
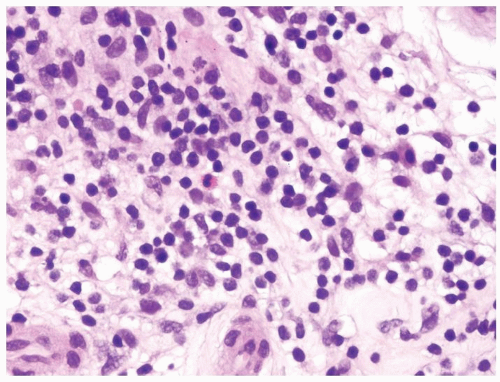 Figure 4.3.4 Idiopathic granulomatous orchitis. Associated chronic inflammation is illustrated with occasional eosinophils admixed with lymphocytes and plasma cells. |
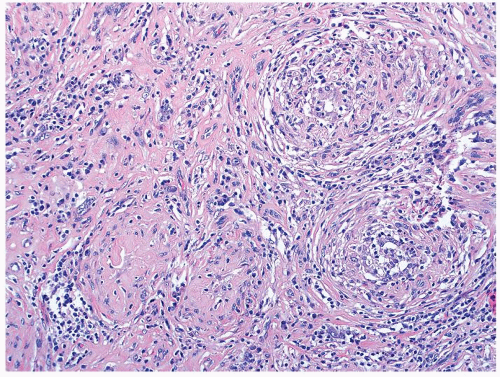 Figure 4.3.5 Idiopathic granulomatous orchitis with scarring. |
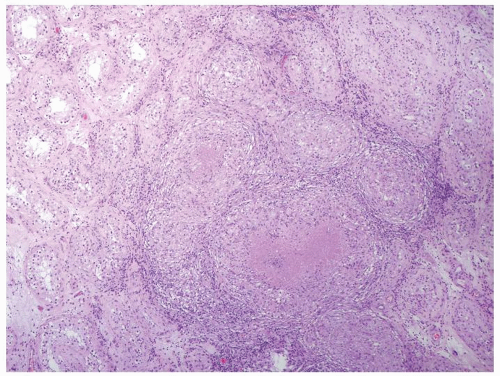 Figure 4.3.6 Mycobacterial granulomatous orchitis. Necrotizing granulomas with palisaded central necrosis is illustrated. |
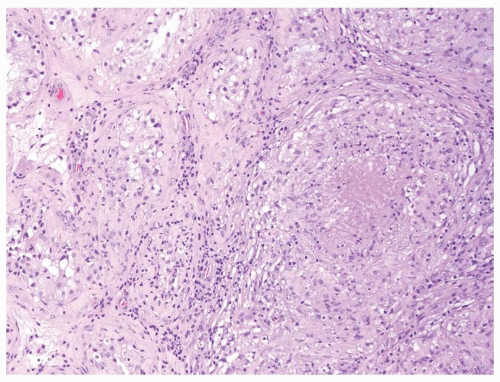 Figure 4.3.7 Mycobacterial granulomatous orchitis. Necrotizing granulomas involve the interstitium with minimal involvement of atrophic seminiferous tubules seen on the left side. |
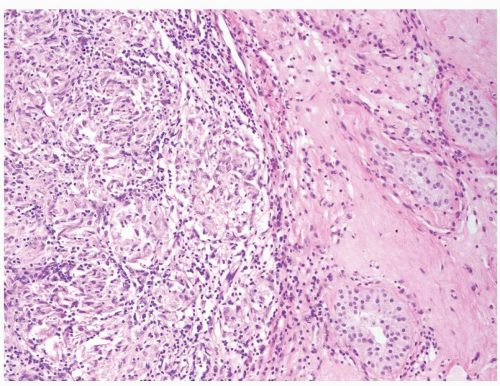 Figure 4.3.8 Nonnecrotizing granulomatous orchitis in sarcoidosis. The process primarily involves the interstitium. |
|
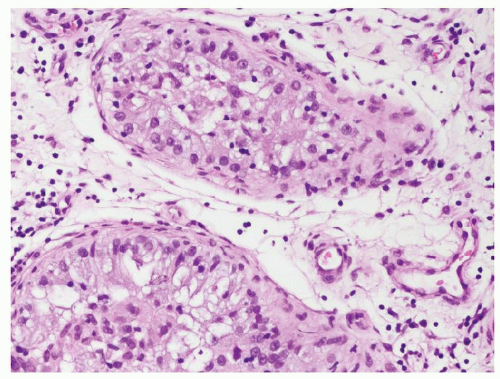 Figure 4.4.1 Idiopathic granulomatous orchitis showing nonnecrotizing granulomas filling seminiferous tubules. Note lack of cytologic atypia in Sertoli cells at periphery of the tubules. |
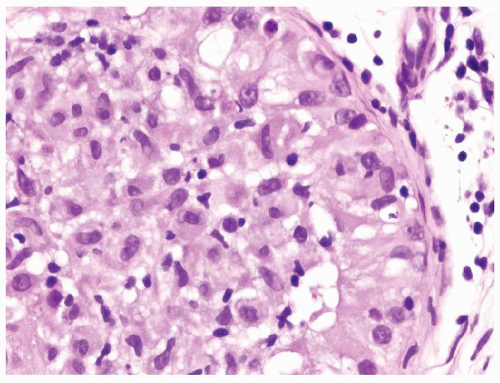 Figure 4.4.2 Idiopathic granulomatous orchitis with a seminiferous tubule filled with epithelioid histiocytes. There is a lack of atypical cells. |
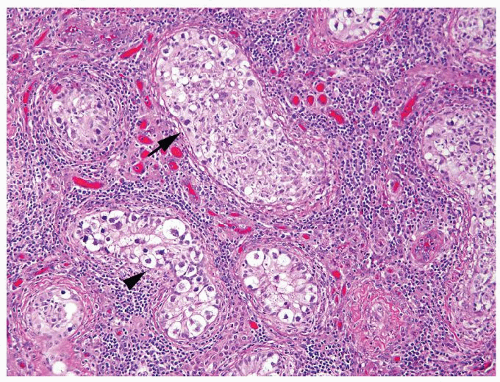 Figure 4.4.3 Some seminiferous tubules with IGCNU not involved with granulomatous response (arrowhead). Other tubules have granulomatous inflammation within the tubules involved by IGCNU (arrow). |
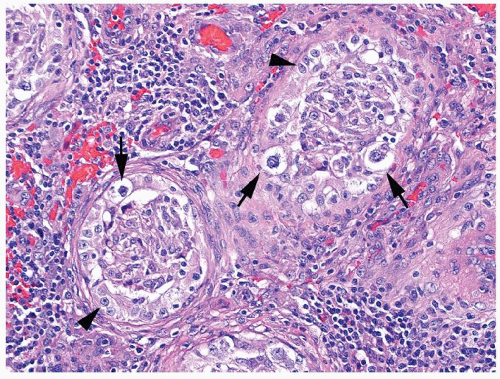 Figure 4.4.4 Nonnecrotizing granulomas involving some seminiferous tubules in association with IGCNU. Note the presence of highly atypical precursor neoplastic cells at the periphery of the tubules with typical cleared cytoplasm and coarse chromatin (arrows). Contrast with Sertoli cells with smaller, uniform, round-oval shape, uniform chromatin, and a single central nucleolus (arrowheads). |
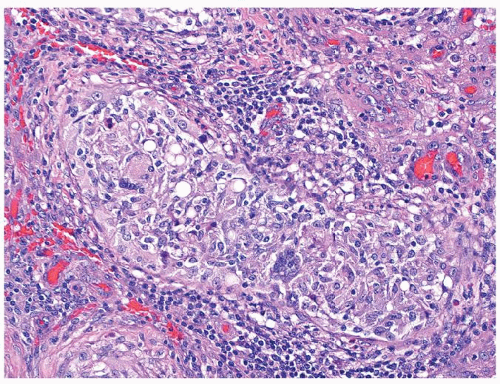 Figure 4.4.5 Nonnecrotizing granulomas in association with IGCNU (same case as in Figure 4.4.4) with extensive intratubular granulomatous reaction destroying IGCNU cells, mimicking idiopathic granulomatous orchitis. |
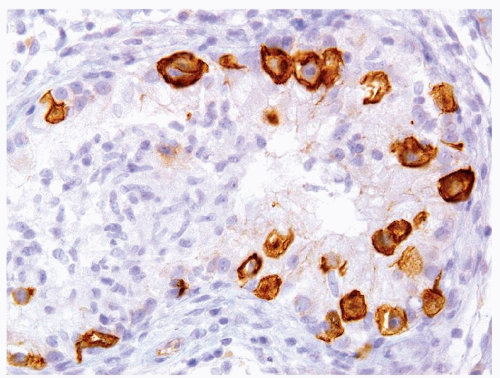 Figure 4.4.6 Nonnecrotizing granulomas in association with IGCNU highlighted by CD117. |
|
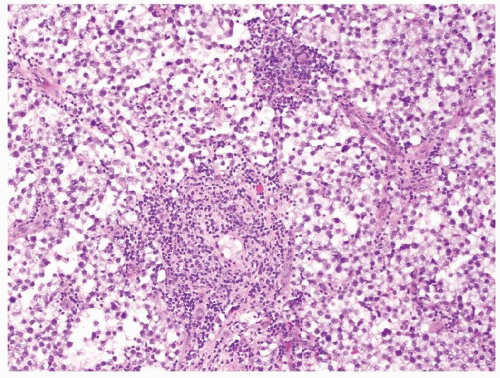 Figure 4.5.1 Focal nonnecrotizing interstitial granulomatous inflammation composed of histiocytes is seen in septae dividing sheets of seminoma cells. |
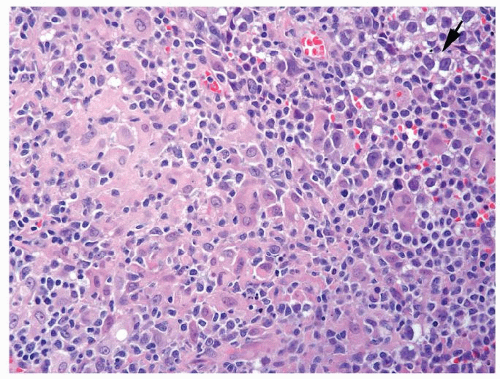 Figure 4.5.2 Rare seminoma cells (arrow) associated with extensive nonnecrotizing interstitial granulomatous inflammation composed of epithelioid histiocytes admixed with lymphocytes, plasma cells, and multinucleated histiocytes. |
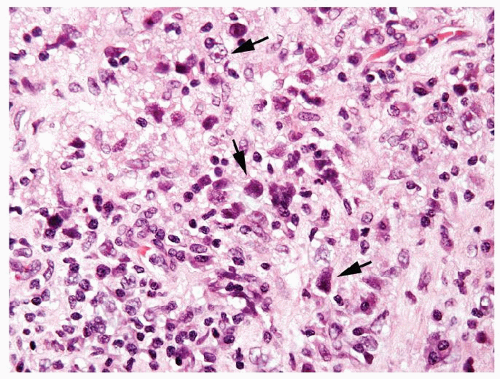 Figure 4.5.3 Rare seminoma cells (arrows) associated with extensive nonnecrotizing interstitial granulomatous inflammation. Some seminoma cells are very hyperchromatic where it is difficult to see nuclear detail as these cells are fragile and can show crush artifact. Others have preserved prominent nucleoli. |
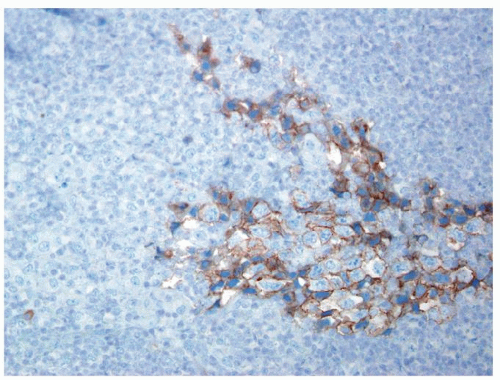 Figure 4.5.4 Seminoma cells labeled with PLAP immunostain. |
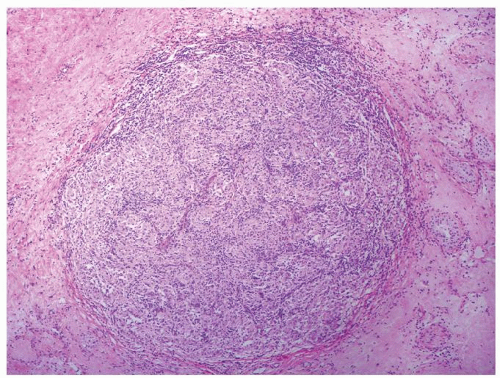 Figure 4.5.5 Nonnecrotizing granulomatous orchitis in sarcoidosis composed of well-formed granulomas. Note surrounding scarring and atrophic seminiferous tubules lacking IGCNU. |
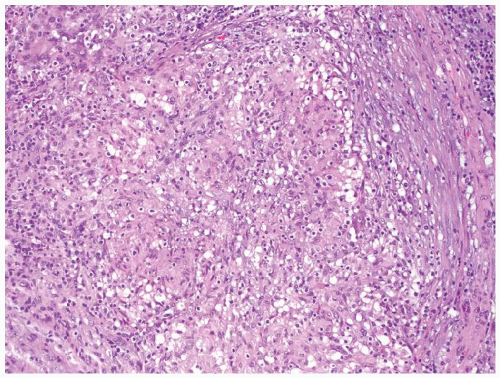 Figure 4.5.6 Mycobacterial granulomatous orchitis with discrete granuloma. |
|
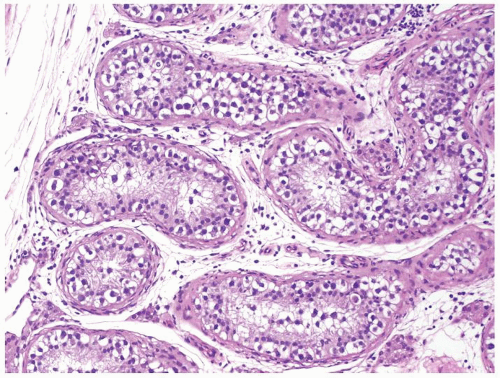 Figure 4.6.1 Seminiferous tubules contain IGCNU. Enlarged, atypical germ cells with cytoplasmic clearing in a single row along a thickened basement membrane are noted. |
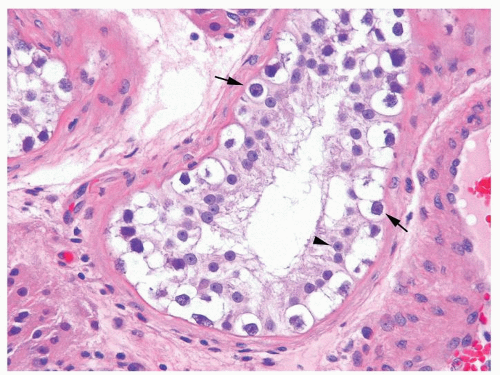 Figure 4.6.2 Seminiferous tubules contain IGCNU with enlarged hyperchromatic nuclei with coarse chromatin residing as a single row along a thickened basement membrane (arrows). Sertoli cell nuclei are smaller with more uniform chromatin and a single small central nucleolus (arrowhead). |
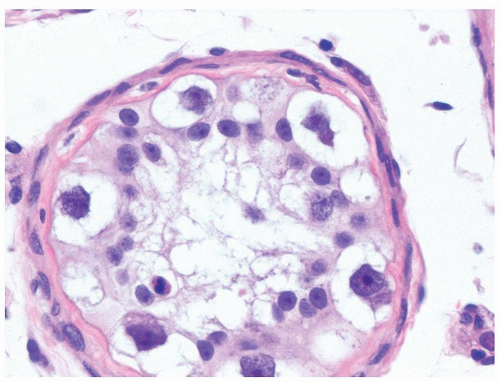 Figure 4.6.3 IGCNU cells have clear cytoplasm, irregular nuclear contours, coarse chromatin, and enlarged single or multiple enlarged variably sized nucleoli. |
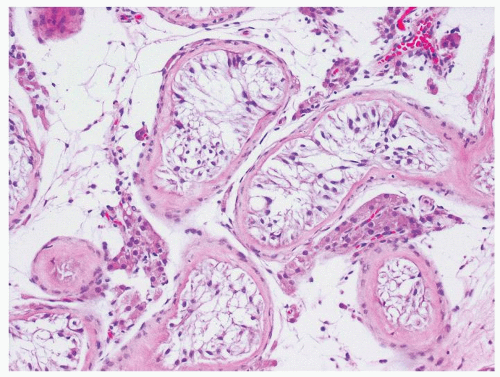 Figure 4.6.4 Seminiferous tubules contain only Sertoli cells. Cells at low power often have a wispy appearance. Peritubular fibrosis is common. |
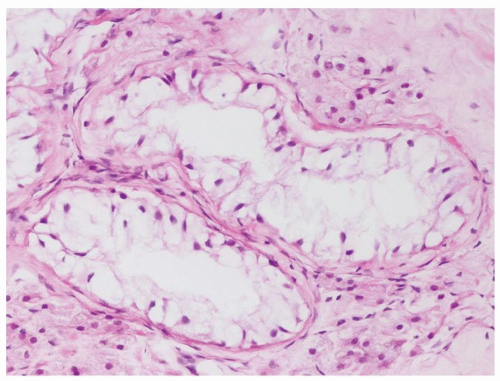 Figure 4.6.5 Seminiferous tubules contain only Sertoli cells with small bland nuclei and abundant vacuolated cytoplasm. |
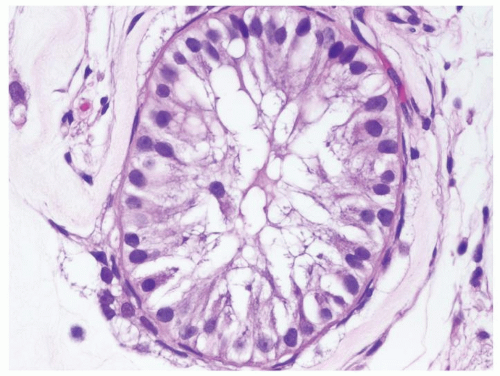 Figure 4.6.6 Seminiferous tubules contain only Sertoli cells. Nuclei are round-to-ovoid with a smooth outline, uniform chromatin and small uniform nucleoli. |
|
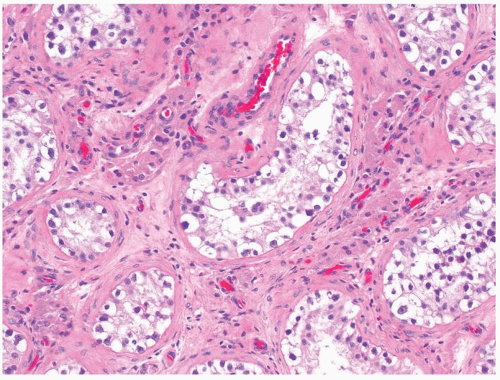 Figure 4.7.1 Seminiferous tubules contain IGCNU. Enlarged, atypical germ cells are situated as a single row along a thickened basement membrane. |
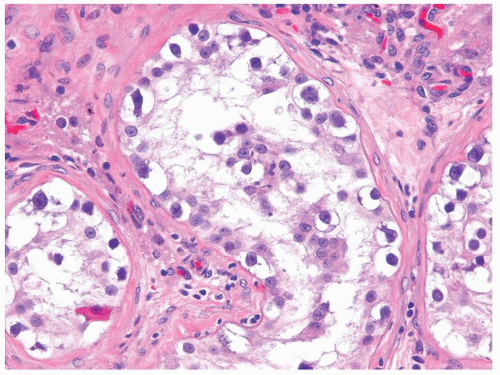 Figure 4.7.2 IGCNU cells have clear cytoplasm, irregular nuclear contours, coarse chromatin, and enlarged single or multiple enlarged variably sized nucleoli. |
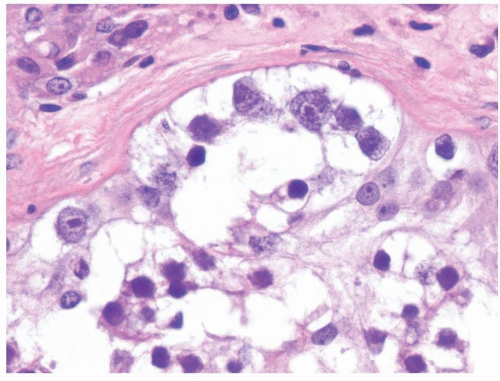 Figure 4.7.3 IGCNU cells with irregular nuclear contours and coarse chromatin. |
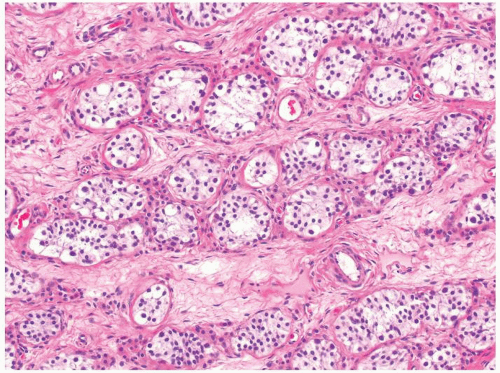 Figure 4.7.4 Spermatogonia with clear cytoplasm containing small-size nuclei with round and regular nuclear contours are seen in this prepubertal testis. |
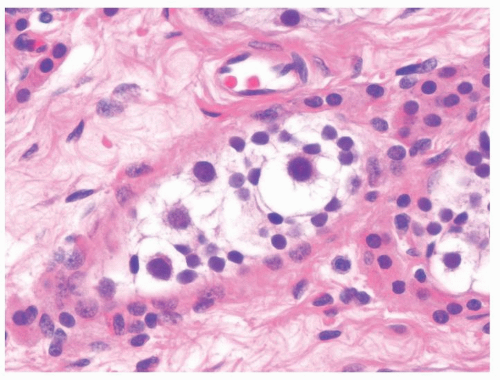 Figure 4.7.5 Occasional spermatogonia in the prepubertal testes may increase in size but maintain regular nuclear contour. The lack of atypia distinguishes these giant spermatogonia from IGCNU. |
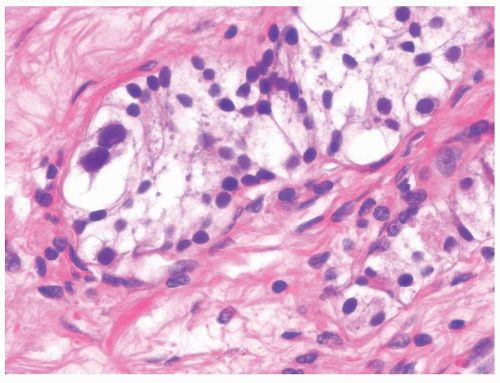 Figure 4.7.6 Spermatogonia with clear cytoplasm containing small-size nuclei with round and regular nuclear contours are seen with occasional binucleated giant spermatogonia in this prepubertal testis. The lack of nuclear atypia and prominent nucleoli are helpful features. |
|
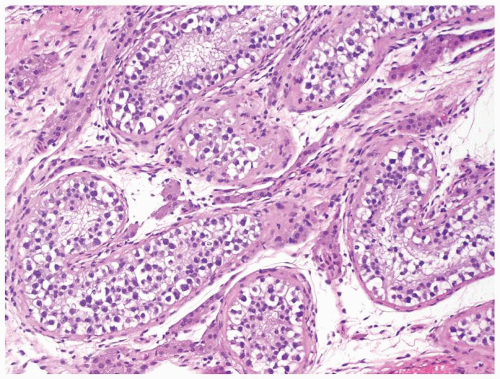 Figure 4.8.1 Seminiferous tubules contain IGCNU. |
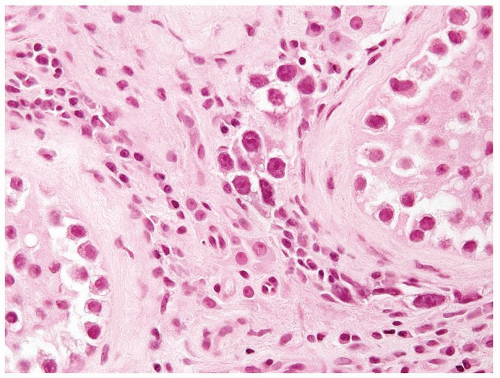 Figure 4.8.2 Intertubular/interstitial invasive seminoma component adjacent to the seminiferous tubule with IGCNU. |
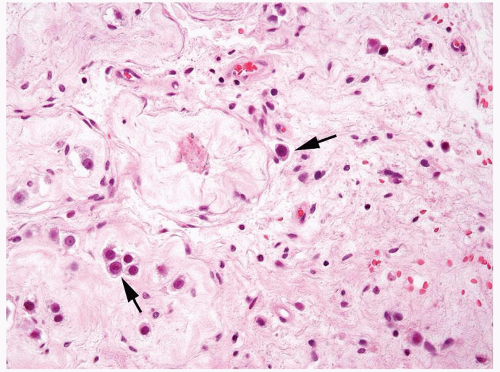 Figure 4.8.3 Intertubular/interstitial invasive seminoma (arrows) adjacent to sclerotic seminiferous tubules. |
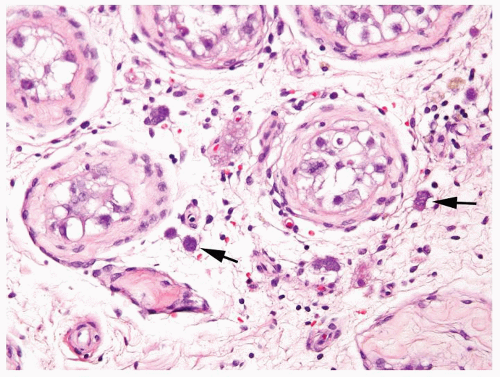 Figure 4.8.4 Intertubular/interstitial invasive seminoma (arrows) permeating the testicular stroma between the seminiferous tubule with IGCNU. |
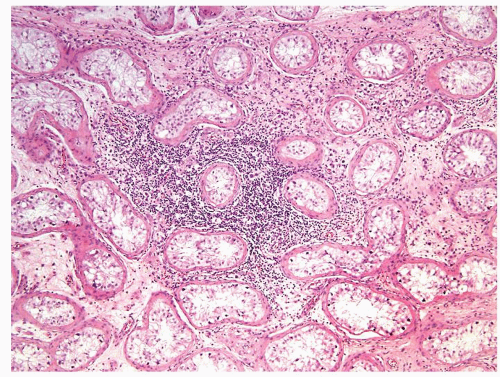 Figure 4.8.5 Associated lymphoplasmacytic infiltrate is a clue raising the suspicion for the presence of an invasive component. |
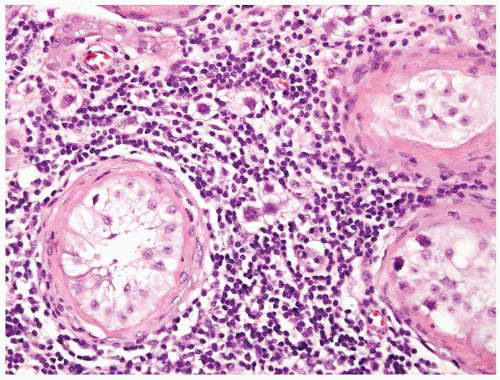 Figure 4.8.6 Same case as Figure 4.8.5 with intertubular invasive neoplastic seminoma cells in lymphoplasmacytic infiltrate. |
|
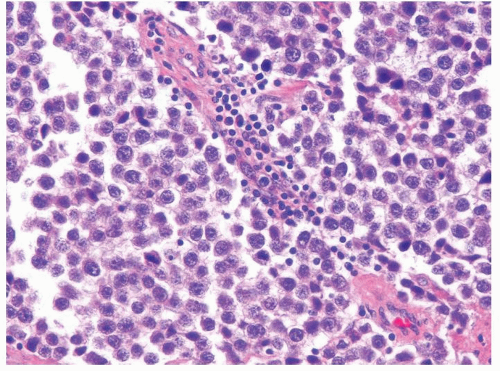 Figure 4.9.1 Classic seminoma composed of monotonous round-to-polygonal cleared cells with ovoid nuclei containing one or more prominent nucleoli with scattered interstitial lymphocytic infiltrate. |
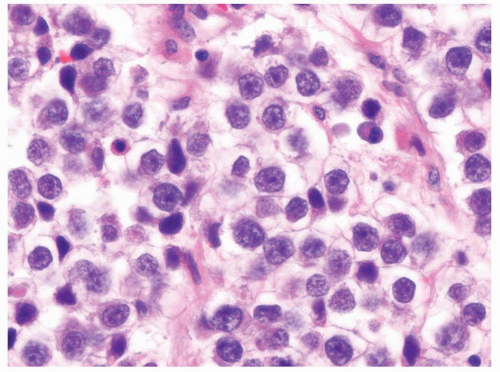 Figure 4.9.2 Monotonous round-to-polygonal cleared cells with ovoid nuclei typical of classic seminoma. |
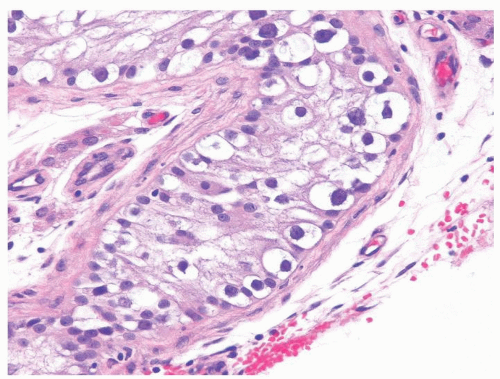 Figure 4.9.3 IGCNU is invariably present in seminiferous tubules associated with classic seminoma. |
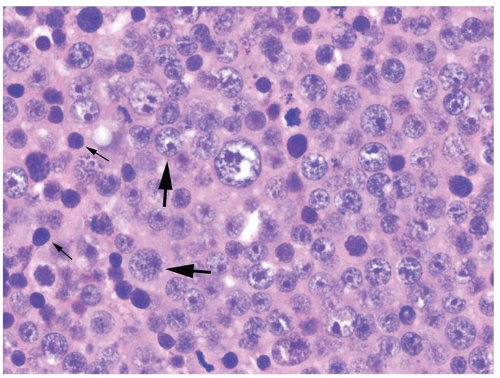 Figure 4.9.4 Spermatocytic seminoma with three cell types: (1) predominant round, intermediate-size cells with characteristic lacy filamentous chromatin (large arrows); (2) smaller cells with dark nuclei and scant cytoplasm (small arrows); and (3) large mononucleated or multinucleated giant cells (center). Note eosinophilic cytoplasm. |
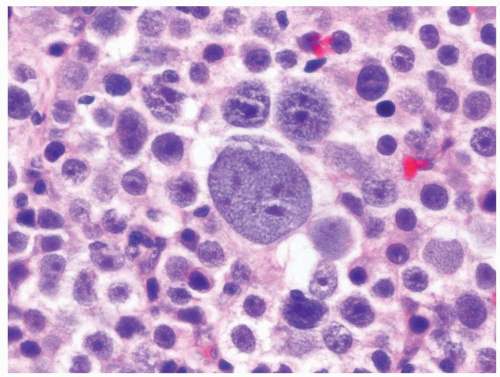 Figure 4.9.5 Spermatocytic seminoma is composed of three basic cell types. Lymphocytic host response is lacking. |
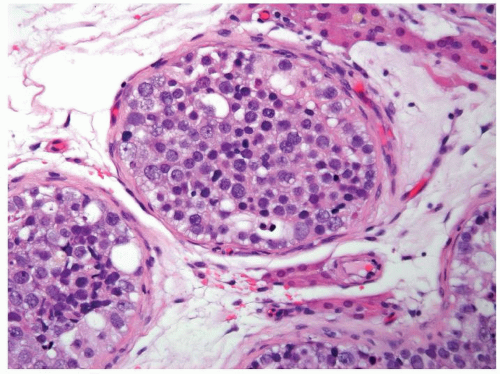 Figure 4.9.6 Intratubular spermatocytic seminoma with the same three basic cell types filling seminiferous tubules. |
|
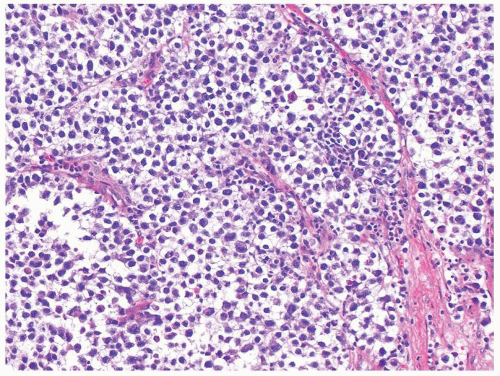 Figure 4.10.1 Classic seminoma is composed of loosely cohesive monotonous round-to-polygonal cells with clear cytoplasm. |
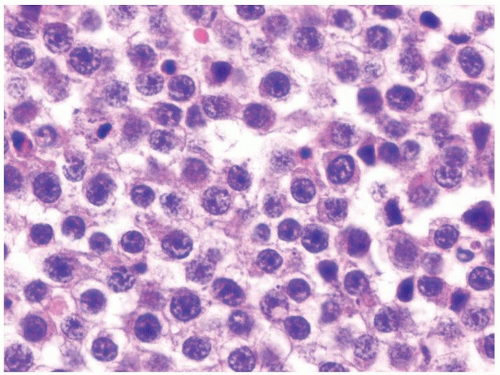 Figure 4.10.2 Relatively uniform nuclei with central prominent nucleoli. |
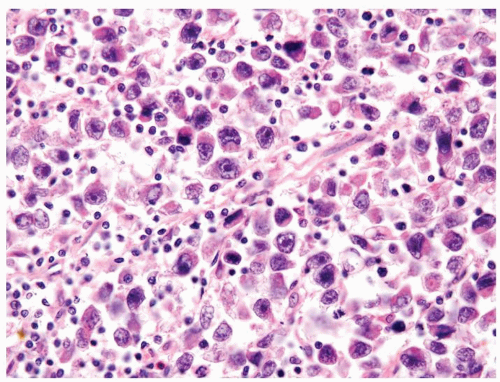 Figure 4.10.3 Seminoma with greater than usual pleomorphism. Cells are still loosely cohesive with interspersed lymphocytes. |
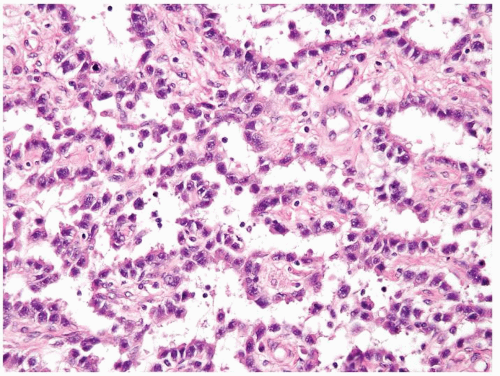 Figure 4.10.4 Seminoma with pseudoalveolar pattern. Cells are still typical of seminoma. |
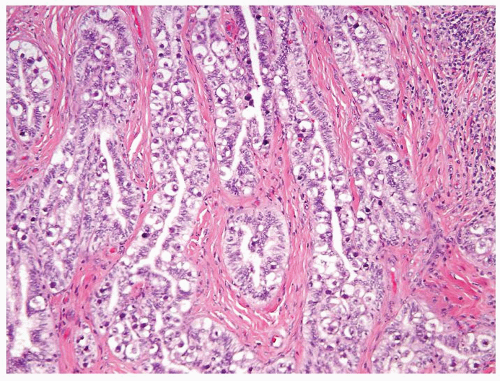 Figure 4.10.5 Seminoma with pagetoid spread into the rete testis. |
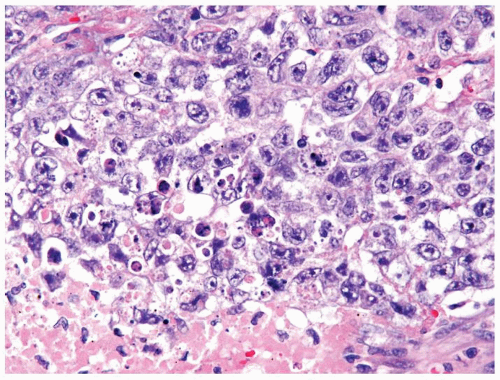 Figure 4.10.6 Embryonal carcinoma composed of large polygonal cells with abundant granular amphophilic cytoplasm and large vesicular irregular nuclei with one or more irregular nucleoli. |
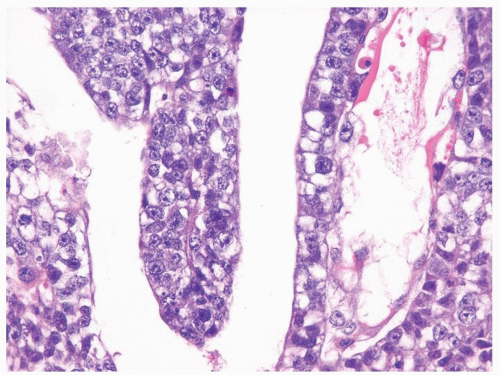 Figure 4.10.7 Embryonal carcinoma cohesive cells and focal area with clear cytoplasm. |
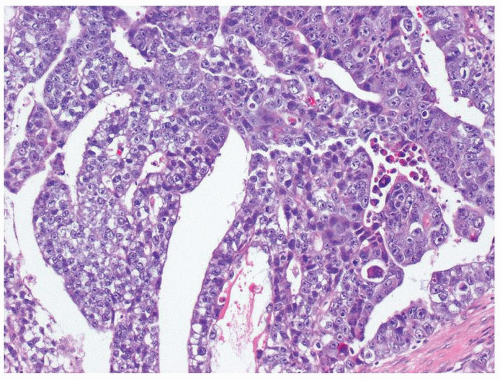 Figure 4.10.8 Embryonal carcinoma with clefts and gland-like structures. |
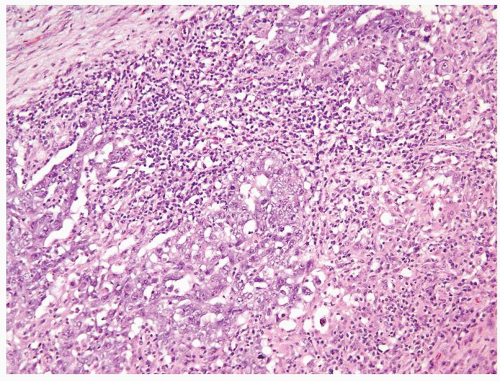 Figure 4.10.9 Unusual embryonal carcinoma with lymphocytic infiltrate. Cells are cohesive with clefts. |
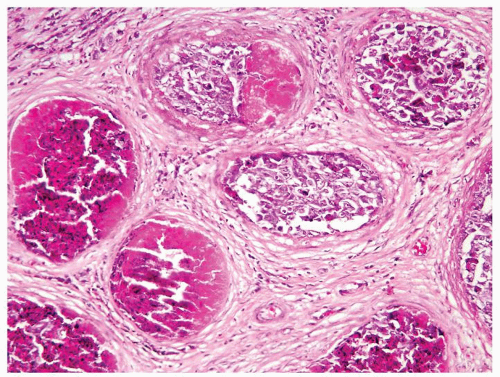 Figure 4.10.10 Intratubular embryonal carcinoma with eosinophilic necrosis. |
|
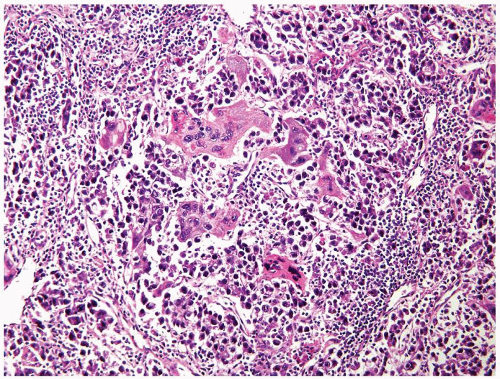 Figure 4.11.1 Seminoma admixed with syncytiotrophoblasts, which are multinucleated cells that contain abundant basophilic cytoplasm. No cytotrophoblasts are accompanied. |
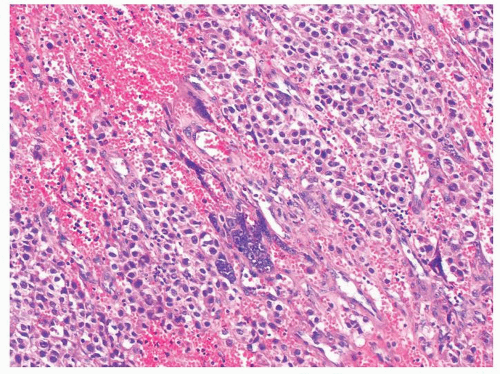 Figure 4.11.2 Syncytiotrophoblasts without associated cytotrophoblasts are seen adjacent to areas of hemorrhage in seminoma. |
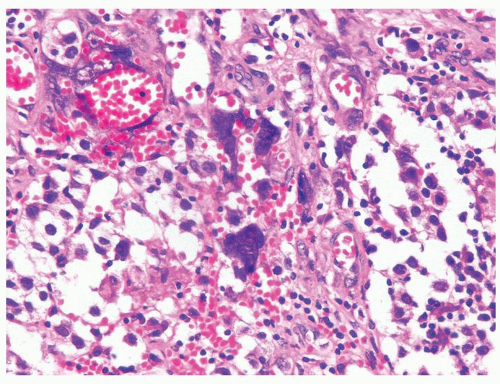 Figure 4.11.3 Syncytiotrophoblasts without associated cytotrophoblasts are seen surrounding vascular structures in seminoma. |
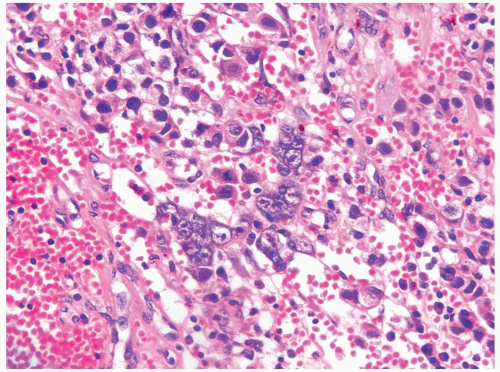 Figure 4.11.4 Syncytiotrophoblasts without associated cytotrophoblasts are seen adjacent to areas of hemorrhage in seminoma. |
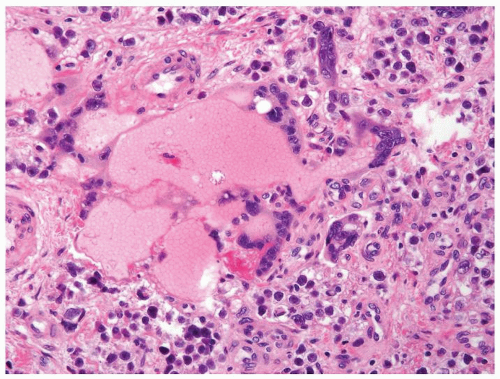 Figure 4.11.5 Syncytiotrophoblasts without associated cytotrophoblasts are seen surrounding vascular structures in seminoma. |
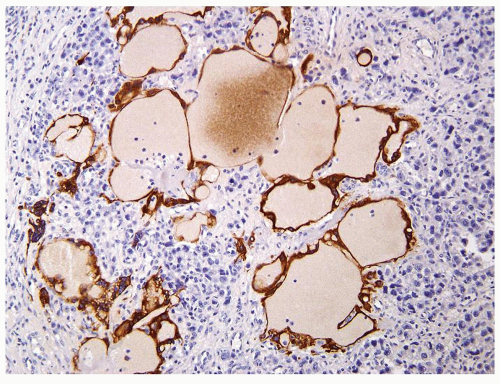 Figure 4.11.6 Same case as in Figure 4.11.5 with highlighting of syncytiotrophoblasts by HCG immunostains. |
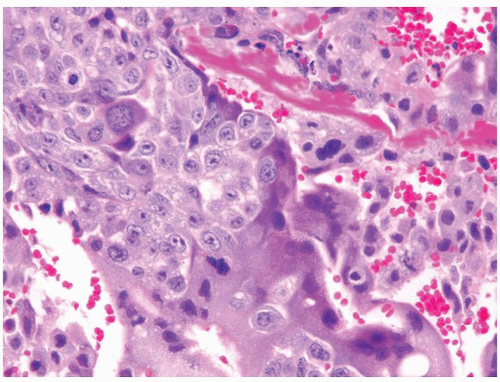 Figure 4.11.7 Cytotrophoblasts are intimately admixed with syncytiotrophoblasts in choriocarcinoma. |
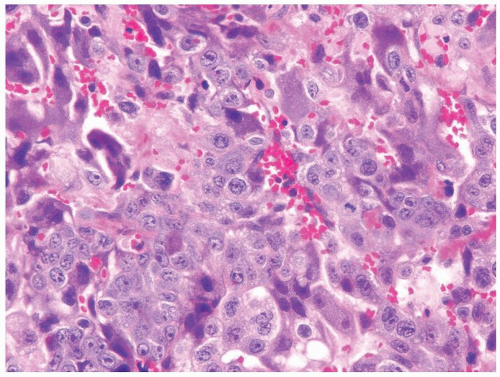 Figure 4.11.8 Cytotrophoblasts are intimately admixed with smaller syncytiotrophoblasts with amphophilic cytoplasm in choriocarcinoma. Cytotrophoblasts have paler cytoplasm surrounding an irregular, single nucleus with one or more nucleoli. |
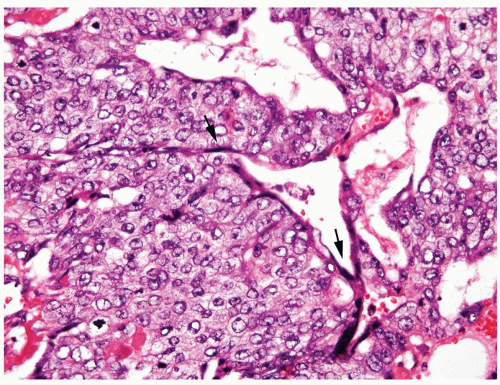 Figure 4.11.9 Choriocarcinoma with subtle syncytiotrophoblasts (arrows) enveloping cytotrophoblasts. |
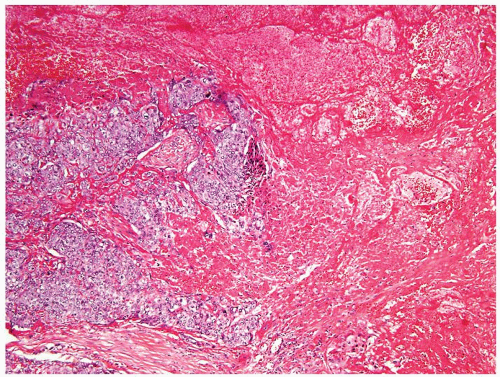 Figure 4.11.10 Choriocarcinoma with extensive hemorrhage and necrosis. |
|
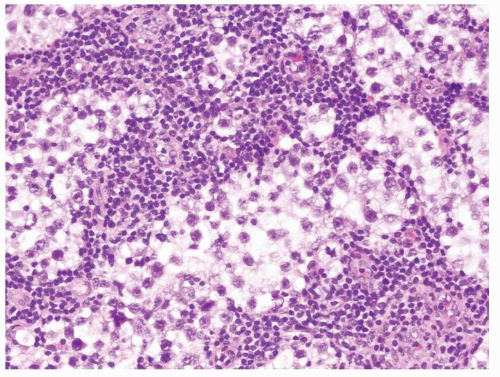 Figure 4.12.1 Classic seminoma composed of sheets of back-to-back monotonous neoplastic cells separated with associated lymphocytic infiltrate. |
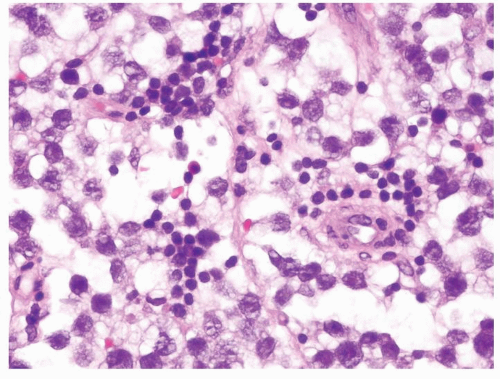 Figure 4.12.2 Classic seminoma with relatively uniform round-to-polygonal cleared cells with ovoid nuclei. |
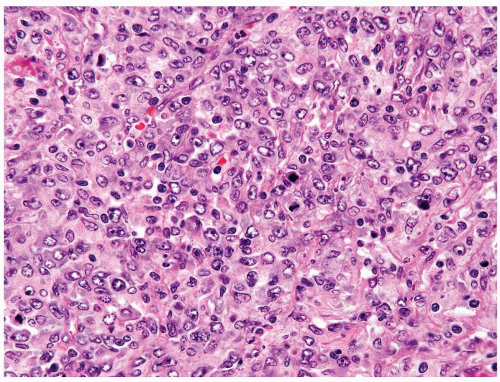 Figure 4.12.3 Large cell lymphoma with cells showing more pleomorphism than seminoma. Also the cells lack central prominent nucleoli in the majority of cells. |
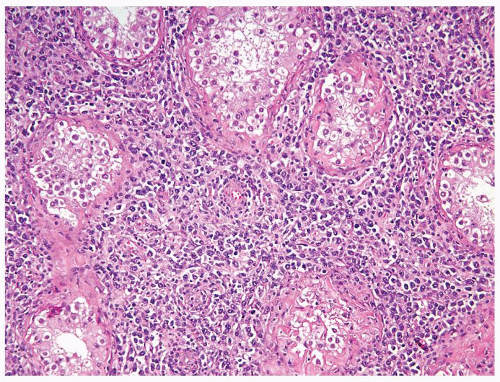 Figure 4.12.4 Lymphoma with relative preservation of testicular architecture. |
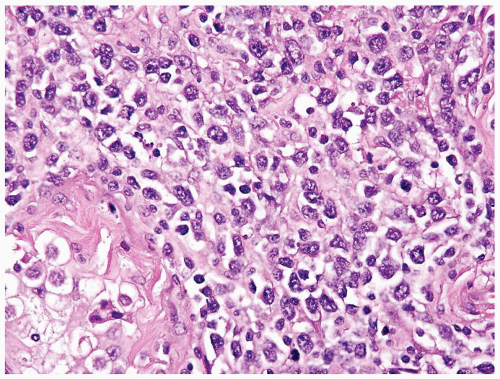 Figure 4.12.5 Large cell lymphoma with less uniformity than seminoma. Also the cells lack central prominent nucleoli in the majority of cells. |
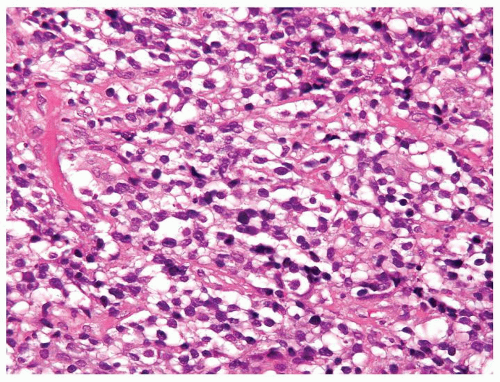 Figure 4.12.6 Lymphoma with clear cytoplasm. Cells lack vesicular nuclei with prominent nucleoli. |
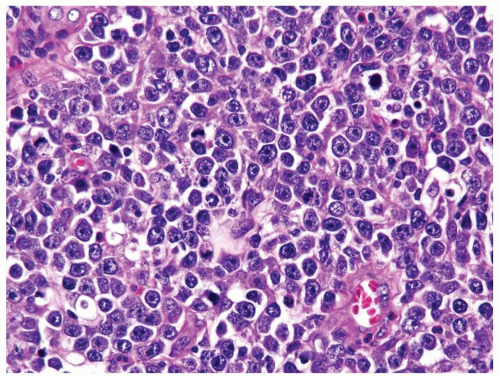 Figure 4.12.7 Lymphoma mimicking seminoma with prominent nucleoli, yet cells have amphophilic cytoplasm. |
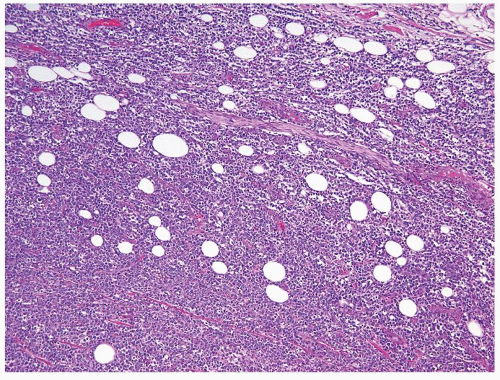 Figure 4.12.8 Lymphoma spread outside of the testis with entrapment of adipocytes. |
|
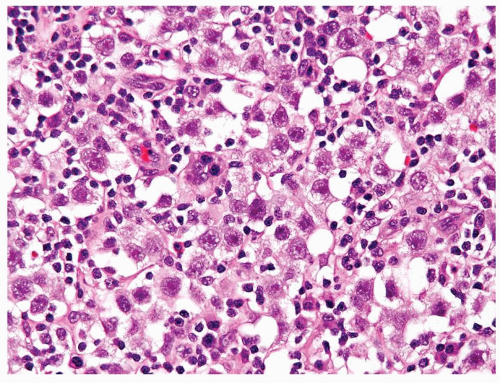 Figure 4.13.1 Classic seminoma is composed of monotonous round-to-polygonal cleared cells with lymphocytic infiltrate. |
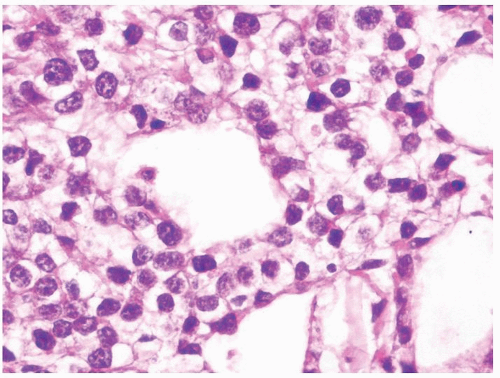 Figure 4.13.2 Classic seminoma with pseudoglandular spaces with uniform, loosely cohesive seminoma cells. |
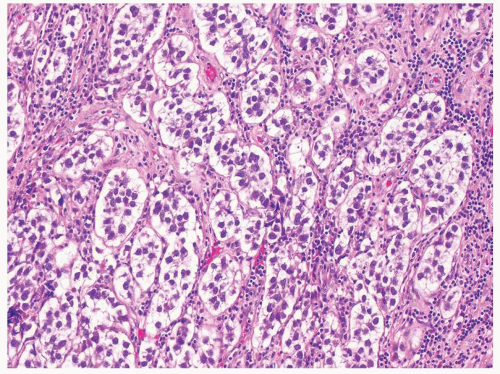 Figure 4.13.3 Classic seminoma with nesting appearance. |
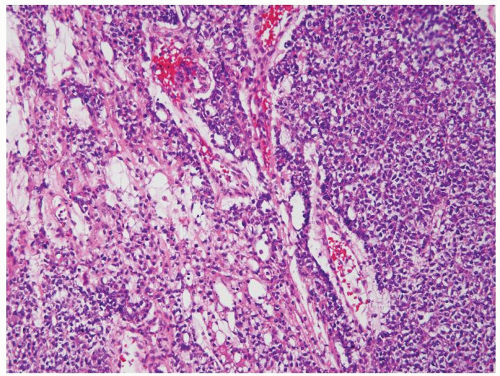 Figure 4.13.4 Yolk sac tumor composed of sheets of cells (right) with a more typical microcystic component (left). |
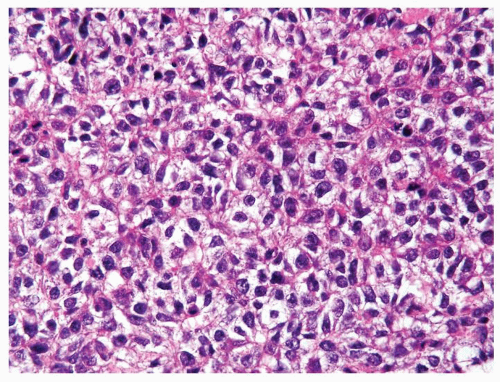 Figure 4.13.5 Same case as Figure 4.13.4 with cells mimicking seminoma, however lacking the seminoma cells’ uniform shape, vesicular nuclei, and large prominent eosinophilic nucleoli. |
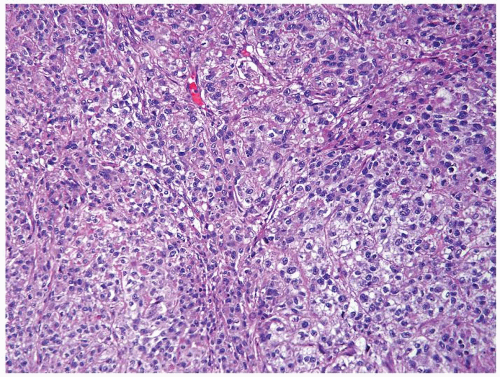 Figure 4.13.6 Solid yolk sac tumor. |
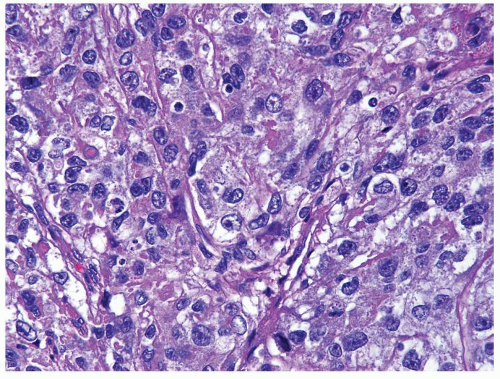 Figure 4.13.7 Same case as Figure 4.13.6 with polygonal, medium-sized, cells with clear to eosinophilic cytoplasm and variably shaped nuclei. |
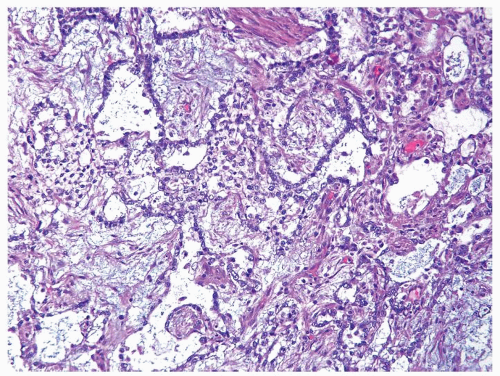 Figure 4.13.8 Same case as Figures 4.13.6 and 4.13.7 with more typical myxoid features. |
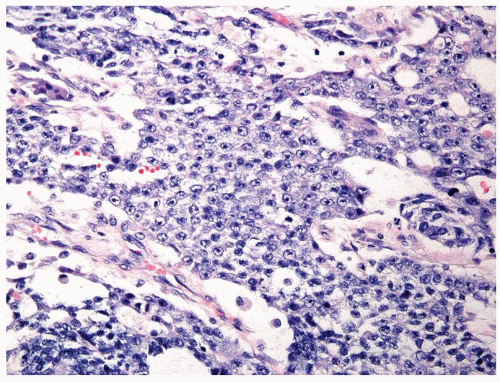 Figure 4.13.9 Solid yolk sac tumor, which is more cohesive than seminoma. |
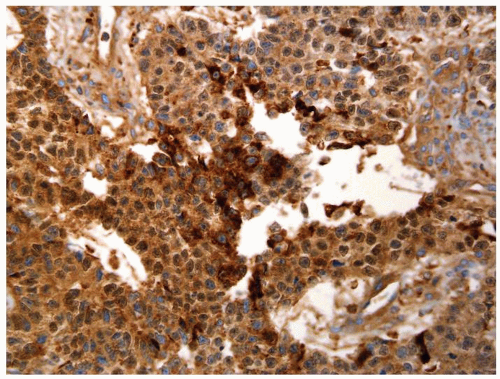 Figure 4.13.10 Same case as Figure 4.13.9 with diffuse positivity for AFP. |
|
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


