Syringocystadenoma Papilliferum
Steven D. Billings, MD
Key Facts
Clinical Issues
Approximately 1/2 present at birth or childhood
Scalp most common location, followed by face
Often associated with nevus sebaceus (present in 5-19% of cases of nevus sebaceus)
Benign tumors, but
Rarely, basal cell carcinoma may develop within syringocystadenoma papilliferum
Rare cases may transform to syringocystadenocarcinoma papilliferum
Microscopic Pathology
Endophytic/exophytic adnexal tumors
Invaginations that communicate with epidermal surface
Invaginations have papillary architecture
Papillary structures lined by glandular epithelium with a double layer
Papillae communicate with duct-like structures in deeper aspects
Basal layer is flattened to cuboidal
Luminal layer usually columnar
Characteristic stroma
Fibrovascular connective tissue within papillae
Numerous plasma cells admixed with some lymphocytes
Top Differential Diagnoses
Hidradenoma papilliferum
Tubular apocrine adenoma
Syringocystadenocarcinoma papilliferum/malignant syringocystadenoma
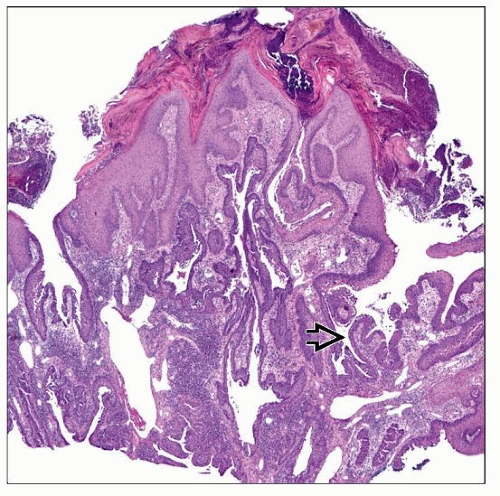 Syringocystadenoma papilliferum has an endo/exophytic growth pattern with invaginations into the underlying dermis that have a papillary architecture  . . |
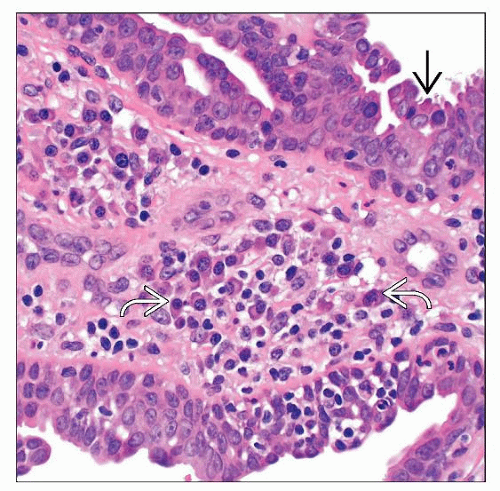 The glandular epithelium in this case shows evidence of apocrine differentiation  , with focal apical snouts and secretions. The stroma contains numerous plasma cells , with focal apical snouts and secretions. The stroma contains numerous plasma cells  . . |
TERMINOLOGY
Abbreviations
Syringocystadenoma papilliferum (SCP)
Definitions
Benign adnexal tumor with endophytic/exophytic growth pattern
ETIOLOGY/PATHOGENESIS
Cytogenetics
Subset of tumors have loss of heterozygosity for PTCH &/or P16, suggesting a role for loss of these tumor suppressor genes in some cases
CLINICAL ISSUES
Epidemiology
Age
Approximately 1/2 present at birth or childhood
Presentation
Scalp most common location, followed by face
Presents as solitary gray to dark brown papillomatous lesion
Rarely multiple
Often associated with nevus sebaceus (present in 5-19% of cases of nevus sebaceus)
Typically in scalp lesions
May rarely be associated with other neoplasms (e.g., tricholemmoma, apocrine hidrocystoma)
Treatment
Surgical approaches
Simple excision is curative
Prognosis
Benign
Rare cases may have a basal cell carcinoma develop within the syringocystadenoma papilliferum
Rare cases may transform to syringocystadenocarcinoma papilliferum
MICROSCOPIC PATHOLOGY
Histologic Features
Endo-/exophytic tumors
Invaginations that communicate with epidermal surface
Superficial aspects often lined by squamous epithelium that transitions to glandular epithelium
Invaginations have papillary architecture
Papillary structures lined by glandular epithelium with a double layer
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


