Suspicious for Hürthle Cell Neoplasm
Mojgan Amrikachi, MD
Key Facts
Clinical Issues
3-15% of thyroid neoplasms
F:M = 3:1
Cytopathology
Crowded groups, small clusters, or dyscohesive cells
Polygonal cells with abundant granular cytoplasm, large round nuclei, and prominent nucleoli
Thyroglobulin (+), high molecular weight keratin (+), TTF-1(+), CK5/6(+)
Top Differential Diagnoses
Adenomatous nodules with Hürthle cell hyperplasia, PTC, MTC, lymphocytic thyroiditis
Reporting Considerations
Aspirate with abundant Hürthle cells and scattered lymphocytes or some watery colloid is best diagnosed as atypia of undetermined significance
Anisonucleosis, atypia, and nuclear irregularity are not reliable features for diagnosis of malignancy
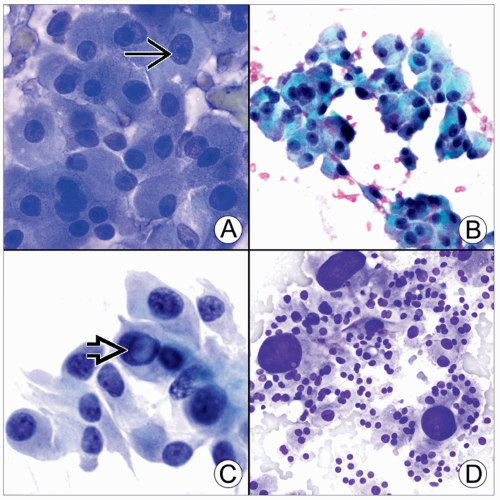 (A) Diff-Quik stain shows Hürthle cells with granular cytoplasm due to intracytoplasmic accumulation of mitochondria. Nuclei are round and have prominent nucleoli  . (B) Pap stain of a Hürthle cell nodule shows 3D groups of oncocytic cells with microfollicular architecture. Cells have blue-green cytoplasm and eccentric nuclei. (C) Pap stain illustrates Hürthle cells with reactive changes. There is marked size variability and a nuclear pseudoinclusion . (B) Pap stain of a Hürthle cell nodule shows 3D groups of oncocytic cells with microfollicular architecture. Cells have blue-green cytoplasm and eccentric nuclei. (C) Pap stain illustrates Hürthle cells with reactive changes. There is marked size variability and a nuclear pseudoinclusion  , mimicking papillary carcinoma. (D) Diff-Quik stain shows Hürthle cells with small cell dysplasia and large cell dysplasia, suspicious for Hürthle cell neoplasm. , mimicking papillary carcinoma. (D) Diff-Quik stain shows Hürthle cells with small cell dysplasia and large cell dysplasia, suspicious for Hürthle cell neoplasm. |
TERMINOLOGY
Abbreviations
Suspicious for follicular neoplasm, Hürthle cell type (SFNHT); suspicious for Hürthle cell neoplasm (SHN)



