is also the etiologic agent of cat scratch disease, but other Bartonella species are associated.2 The organism is commonly harbored by domestic cats (which have a seroprevalence of about 5% to >60% depending on geographic area3) and transmitted to their owners. These organisms are susceptible to antibiotics, but untreated disease can prove fatal. Although cutaneous lesions are the most frequently recognized manifestation of bacillary angiomatosis (e-Fig. 17.1), a systemic infection typically ensues in the immunosuppressed host. In immunocompetent individuals, lesions are believed to remain localized to the inoculation site. Bacillary angiomatosis can masquerade as Kaposi sarcoma (KS) in resource-poor areas with a high prevalence of HIV-associated disease.4
TABLE 17.1 Differential Diagnosis of Superficial Vascular Lesions | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
|
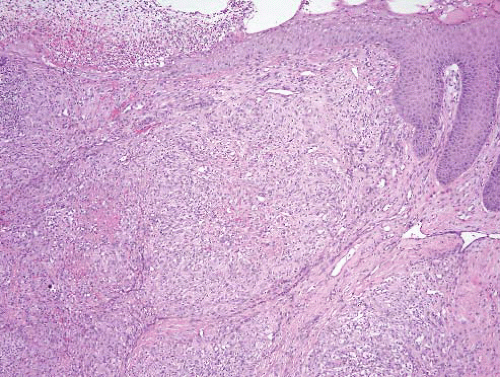 FIGURE 17.1 Bacillary angiomatosis. This lesion arose in the knee area a patient who had had a renal transplant. Beneath the ulcerated skin is a lobular but solid endothelial proliferation. The centers of the lobules contain eosinophilic necrotic material. |
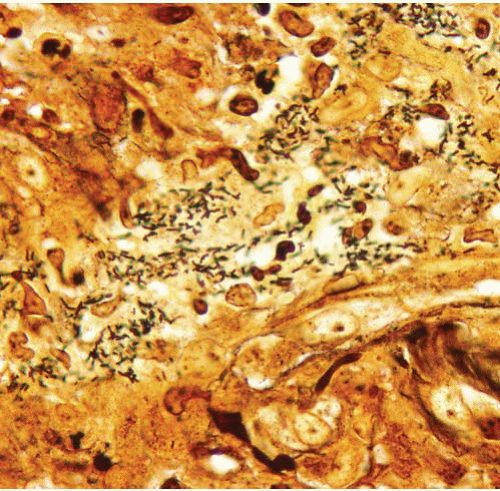 FIGURE 17.2 Bacillary angiomatosis, Warthin-Starry stain. Numerous Bartonella henselae organisms are apparent. |
involving both skin and subcutaneous tissue.7 All contain vasoformation elements, commonly admixed with inflammatory cells and typically arranged in a multinodular or lobulated pattern (Fig. 17.3, e-Figs. 17.10 to 17.13). Superficial examples may be polypoid and, when accompanied by well-formed vessels with patent lumina, may be suggestive of a pyogenic granuloma or bacillary angiomatosis. Lesions which arise in less distensible tissues may exhibit more solid “angioblastic” growth suggestive of a neoplastic process.7 All examples are unified by the presence of plump atypical appearing endothelial (verruga) cells. Depending on the stage of the lesions, lymphocytes and plasma cells or polymorphonuclear leukocytes with microabscess formation may be the predominant inflammatory constituents. Fibrin deposition, cellular necrosis, and fibrosclerosis may also be evident. The identification of Rocha-Lima inclusions, which may be fleeting, assists in confirming the diagnosis. These granular structures are best seen when tissues are fixed in buffered neutral formalin, embedded in glycol methacrylate, and stained with Giemsa.8 They also stain lightly, although less convincingly, with the Warthin-Starry and Periodic acid-Schiff-diastase stains.
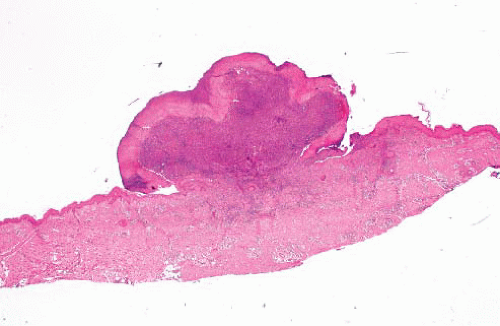 FIGURE 17.3 Verruga peruana. This lesion appears similar to those associated with bacillary angiomatosis; diagnosis requires correlation with the clinical history. (Image courtesy of Dr. Javier Arias-Stella.) |
superficial, firm, bluish or erythematous mass, involving the fingers, head and neck, or anorectal region. Physical examination reveals limited mobility of the process about its longitudinal axis. Astute gross examination by the surgeon or the pathologist may reveal confinement of the process to the lumen of a dilated vessel, usually a vein.
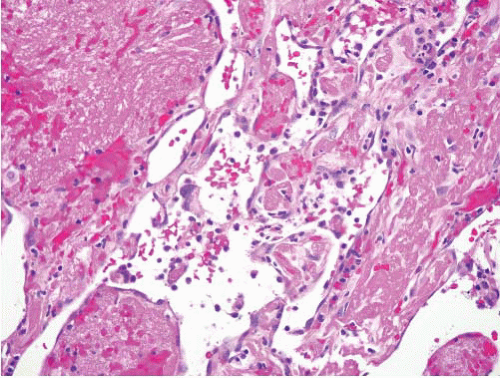 FIGURE 17.4 Papillary endothelial hyperplasia is an exaggerated form of organization of vascular thrombi. Note the fibrin cores coated by a monolayer of endothelial cells. |
Local recurrence has been noted in up to one-third of patients. Whether this is the result of a persisting underlying vascular anomaly (i.e., arteriovenous shunt) or an indication of inherent neoplastic potential is unresolved. Occasional multicentric lesions have been reported. There are no reported deaths due to this process. Optimal management is complete local excision.
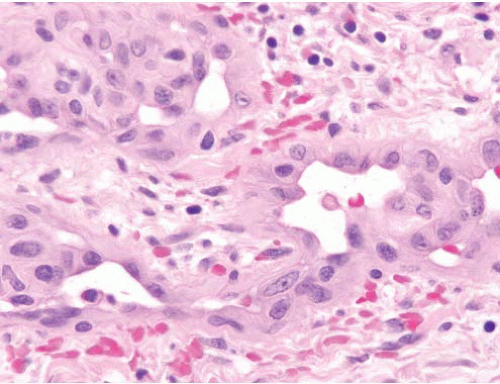 FIGURE 17.5 Angiolymphoid hyperplasia with eosinophilia/epithelioid hemangioma. This lesion shows well-formed vessels lined by plump epithelioid endothelial cells. |
occasionally extending into the dermis, underlying musculature, or adjacent structures such as the salivary glands. Although the microscopic features vary somewhat with the duration of the lesion, all stages feature fibrosis, a reactive vascular proliferation, and an inflammatory infiltrate dominated by eosinophils and lymphocytes (e-Figs. 17.24 to 17.26). Earlier examples typically exhibit a more pronounced inflammatory reaction while later stages are more fibrotic. Lymphoid follicles are a universal finding and are generally distributed through the process. Eosinophilic microabscesses are sometimes present (Fig. 17.7). In contrast to angiolymphoid hyperplasia with eosinophilia (epithelioid hemangioma), the vessels in Kimura disease are typically well canalized, lack epithelioid morphology, and, for the most part, tend to be a relatively minor or inconspicuous component of the process.
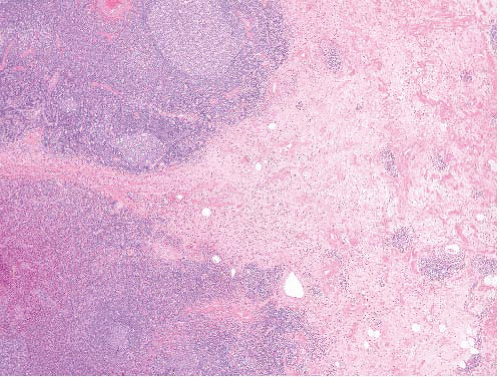 FIGURE 17.6 Kimura disease. Kimura disease is not a vascular lesion but, rather, a fibroinflammatory process. It is included here based on confusion between it and angiolymphoid hyperplasia with eosinophilia/epithelioid hemangioma in the past. |
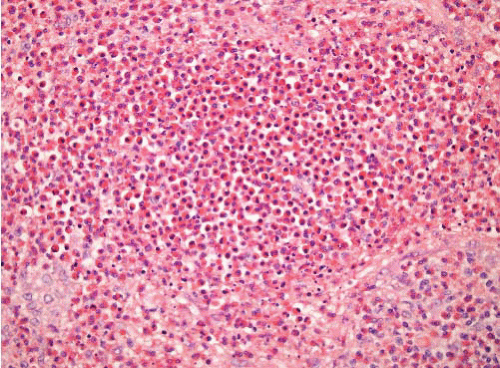 FIGURE 17.7 Kimura disease. Eosinophilic microabscesses are a feature of Kimura disease but not of angiolymphoid hyperplasia with eosinophilia/epithelioid hemangioma. |
pediatric vascular tumors (infantile or juvenile hemangiomas) are often cellular with prominent mitotic activity.
macular stains, including both small, transient lesions (e.g., nevus simplex) and the larger, persistent, port wine stains. Common sites of involvement include the glabella, eyelids, and the nape of the neck. Those located in the center of the face commonly disappear by 1 year of life, whereas nape lesions fade more slowly and often incompletely with faint vestiges persisting into adulthood. Port wine stains (nevus venosus), on the other hand, occur far less frequently. They consist of larger macules with irregular borders which tend to enlarge in proportion to the growth of the child and generally do not fade. They are typically flat in infancy and childhood but may become elevated and nodular later in life.
Maturation is first noted at the periphery of these lobules and is characterized by the presence of flattened or less active appearing endothelium lining vessels with patent lumina. Over time, a greater percentage of the capillaries assume this morphology. The vascular lobules also become more accentuated due to an ingrowth of fibrous and adipose connective tissue.
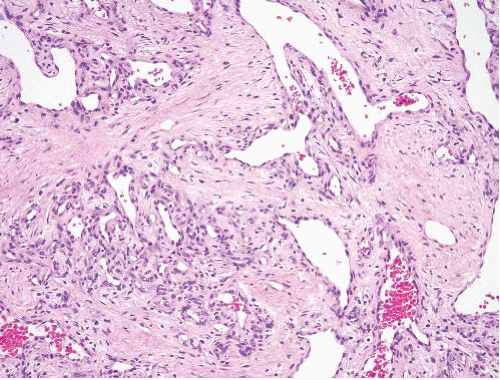 FIGURE 17.8 Capillary hemangioma. This lesion from a small child has a lobular growth pattern, showing larger capillaries branching into smaller ones. The smallest are supported by cells other than endothelial cells (such as myoid cells and pericytes). |
may be sessile, polypoid, or pedunculated. They frequently have a rapid onset but stabilize at a maximum size of several millimeters to a few centimeters after several weeks or months. The lesions range in color from bluish-purple to bright red. Their epithelial surface may be attenuated or ulcerated.
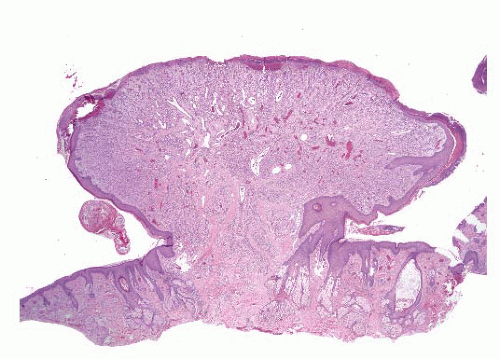 FIGURE 17.9 Pyogenic granuloma (lobular capillary hemangioma). The histologic appearances of these lesions are similar to those of capillary hemangiomas found in infants and small children, but in contrast to those of infants, these are not as likely to regress. Note again the lobular configurations of the proliferating vessels. This example has a collarette of hyperplastic skin. |
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


