Squamous Cell Carcinoma (and Variants)
David Cassarino, MD, PhD
Key Facts
Terminology
Squamous cell carcinoma (SCC)
Malignant epithelial tumor of squamous keratinocytes
Etiology/Pathogenesis
Most cases are related to UV radiation
Previous radiation therapy implicated in some cases, usually associated with more aggressive SCC
Clinical Issues
Often arises in sun-damaged skin of elderly patients (usually head and neck)
Vast majority of cases associated with preexisting actinic keratosis (AK)
Complete surgical excision is optimal and definitive therapy
Prognosis usually good in superficial and well-differentiated cases
Worse prognosis with poorly differentiated, deeply invasive, or aggressive subtypes
Microscopic Pathology
Proliferation of invasive atypical keratinocytes, often with areas of keratinization (keratin pearls) and squamous eddies
Cells are present in nests, sheets, and cords
Cytologically, cells show abundant eosinophilic cytoplasm, and large nucleus with vesicular chromatin and prominent nucleoli
Degree of differentiation is variable, ranging from well- to moderately to poorly differentiated
Multiple variants of differing malignant potential described
 Clinical photograph shows an extensive SCC arising on the distal foot in a patient with a history of previous burn injury. (Courtesy S. Yashar, MD.) |
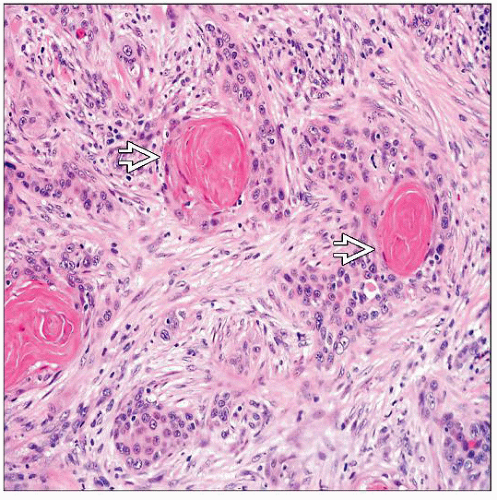 Moderately differentiated invasive SCC shows prominent keratin pearls  and a sclerotic stroma with scattered inflammatory cells. and a sclerotic stroma with scattered inflammatory cells. |
TERMINOLOGY
Abbreviations
Squamous cell carcinoma (SCC)
Synonyms
Epidermoid carcinoma
Sarcomatoid carcinoma/spindle cell carcinoma/carcinosarcoma/metaplastic carcinoma
Acantholytic/adenoid/pseudoglandular SCC
Verrucous carcinoma (well-differentiated variant)
Keratoacanthoma (KA) (well-differentiated variant, regresses spontaneously)
Definitions
Malignant tumor of squamous keratinocytes
ETIOLOGY/PATHOGENESIS
Environmental Exposure
Most cases are related to UV radiation
Some cases are likely related to chronic inflammation (i.e., SCC arising in burns, lupus, lichen planus)
Previous radiation therapy is implicated in some cases, usually associated with more aggressive SCC
Chronic wounds and burn scars also can be associated with high-risk SCC
HPV is associated with some cases
Especially verrucous carcinoma (low grade) and SCC in immunosuppressed patients (high grade)
CLINICAL ISSUES
Epidemiology
Age
Usually in the elderly, especially solar-related lesions
However, can present in a wide age range (34-95 years)
Rare cases in children (should prompt genetic studies)
Gender
Slightly more common in males, overall
Presentation
Slow-growing papular, nodular, or plaque lesion
Often arises in sun-damaged skin (head and neck tumors)
Vast majority of cases associated with preexisting actinic keratosis (AK)
May be ulcerated or bleeding
Ear canal and middle ear tumors may present with pain, hearing loss, and discharge
Treatment
Surgical approaches
Complete surgical excision is optimal and definitive therapy
Mohs surgery has been shown to be highly effective for most tumors
Drugs
If patients are not surgical candidates, topical chemotherapeutics or immunomodulators may be used
Radiation
May be used for very advanced cases where surgical therapy is not curative
Prognosis
Usually excellent in most cases
Worse prognosis with poorly differentiated, deeply invasive, or rare aggressive subtypes
Site of tumor important for prognosis
Lip and ear tumors more aggressive, regardless of degree of differentiation
MACROSCOPIC FEATURES
General Features
Papular to nodular or plaque-like lesion; can be exophytic
May be ulcerated or hemorrhagic
Size
Variable; can be small or large lesions
MICROSCOPIC PATHOLOGY
Histologic Features
Proliferation of invasive atypical keratinocytes
Cells are present in nests, sheets, and infiltrative cords
Often show areas of keratinization (keratin pearls) and squamous eddies
Attachments to overlying epidermis in most cases
Associated AK is very common; less likely, may be associated with SCC in situ (Bowen disease)
Cytologically, cells show abundant eosinophilic cytoplasm and large nucleus with vesicular chromatin and prominent nucleoli
Intercellular bridges (desmosomes) should be present on high-power examination
Presence of dyskeratotic cells (apoptotic keratinocytes) is reliable sign of squamous differentiation
If no definite squamous differentiation is present, immunohistochemistry should be used to confirm diagnosis
Degree of differentiation is variable, ranging from well- to moderately to poorly differentiated
Amount of keratinization typically decreases and cytologic atypia increases with higher grades
Mitotic figures are usually numerous, and atypical forms are found especially in moderately to poorly differentiated cases
Multiple variants of differing malignant potential described
Low-risk variants include well-differentiated SCC arising in AK, keratoacanthoma, verrucous carcinoma, and tricholemmal (variant of clear cell) carcinoma
Intermediate-risk variants include acantholytic (adenoid/pseudoglandular) and lymphoepithelioma-like carcinoma of the skin (LELCS)
High-risk variants include spindle cell/sarcomatoid, basaloid, adenosquamous, and desmoplastic
Also, radiation, burn scar, and immunosuppression-related SCCs
Rare variants of uncertain malignant potential include clear cell SCC, signet ring cell SCC, follicular SCC, papillary SCC, pigmented SCC, and SCC arising from adnexal ducts or cysts
Predominant Pattern/Injury Type
Epithelioid/squamoid
Predominant Cell/Compartment Type
Squamous cell
ANCILLARY TESTS
Immunohistochemistry
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


