Solitary Fibrous Tumor
Key Facts
Clinical Issues
Asymptomatic; incidental finding on routine chest x-ray
Cough
Pleuritic pain
Dyspnea
Hypoglycemia (5% of patients)
Pulmonary osteoarthropathy with clubbing of fingers
Microscopic Pathology
Bland-appearing spindle cell proliferation
Variegation in growth patterns within same tumor
May show prominent myxoid stromal changes
Stroma is highly vascularized with angiofibromatous or hemangiopericytic vascular pattern
Spindle cell areas are variably admixed with areas of stromal hyalinization
Most distinctive pattern of hyalinization is characterized by parallel linear deposits of rope-like collagen separating tumor cells
Oval to spindle cells with scant cytoplasm and oval nuclei with dense chromatin pattern
Very low mitotic activity (1-3 per 10 high-power fields)
Cells are positive for vimentin, CD34, Bcl-2, and CD99
Diagnostic Checklist
Circumscription and encapsulation
Bland-appearing spindle cell proliferation with prominent vascular pattern and variable degrees of stromal sclerosis
Fascicular, short storiform, hemangiopericytic, neural palisading, and synovial sarcoma-like growth patterns
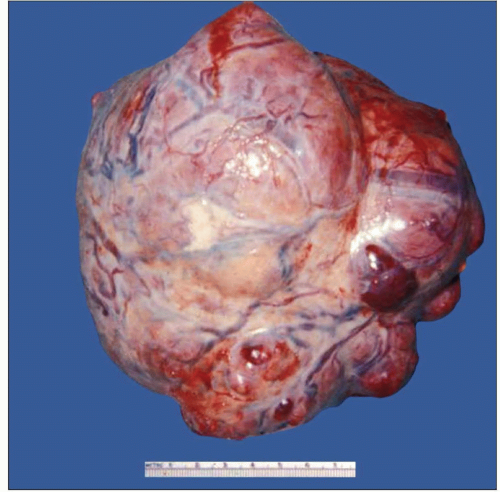 Typical gross appearance of solitary fibrous tumor of the pleura shows a lobulated and well-circumscribed firm mass covered by a thin, shiny capsule with striking vascular markings. |
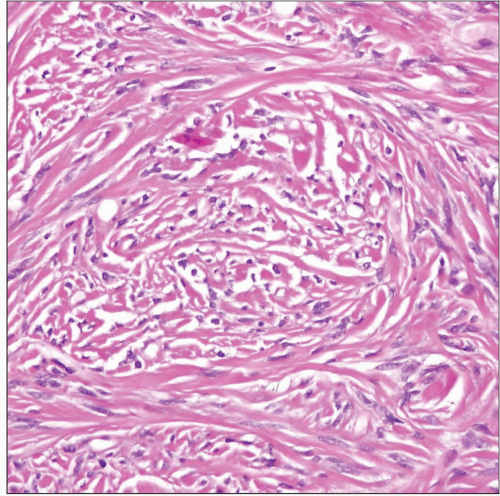 Typical histologic appearance of solitary fibrous tumor of the pleura shows rope-like strands of keloidal collagen flanked by small hyperchromatic spindle cells. |
TERMINOLOGY
Abbreviations
Solitary fibrous tumor (SFT)
Synonyms
Submesothelial fibroma
Fibrous mesothelioma
Localized fibrous tumor
Pleural fibroma
Definitions
Benign neoplastic proliferation of submesothelial fibroblastic cells
ETIOLOGY/PATHOGENESIS
Pathogenesis
Arises from submesothelial fibroblasts
No relationship with asbestos exposure
CLINICAL ISSUES
Presentation
Asymptomatic; incidental finding on routine chest x-ray
Cough
Pleuritic pain
Dyspnea
Hypoglycemia (5% of patients)
Pulmonary osteoarthropathy with clubbing of fingers
Most frequent in adults; no sex predilection
Treatment
Surgical excision
Prognosis
Excellent prognosis following complete excision with clear margins
MACROSCOPIC FEATURES
General Features
Well circumscribed and encapsulated
Sessile, broad-based pleural mass
Pedunculated mass attached to pleural surface by short pedicle
Rubbery, homogeneous, and whorled cut surface
Size: 5-20 cm in greatest diameter
Smooth, shiny outer surface
MICROSCOPIC PATHOLOGY
Histologic Features
Bland-appearing spindle cell proliferation
Variegation in growth patterns
May incorporate entrapped air spaces at interphase with lung parenchyma
May show prominent myxoid stromal changes
May contain metaplastic bone or abnormal “amianthoid” collagen fibers
Stroma is highly vascularized with angiofibromatous or hemangiopericytic vascular pattern
Spindle cell areas are variably admixed with areas of stromal hyalinization
Most distinctive pattern of hyalinization is characterized by parallel linear deposits of rope-like collagen separating tumor cells
Areas with degeneration of collagen may simulate tumor cell necrosis
Cytologic Features
Oval to spindle cells with scant cytoplasm and oval nuclei with dense chromatin pattern
Spindle cells may show wavy nuclei resembling schwannian cells
Multinucleated giant cells may be present
Very low mitotic activity (1-3 per 10 high-power fields)
ANCILLARY TESTS
Immunohistochemistry
Cells are positive for vimentin, CD34, Bcl-2, and CD99
Focal positivity has been reported in some cases for cytokeratin and SMA; otherwise negative for all other markers
Diagnosis of exclusion; CD34 positivity is not exclusive for this tumor and may be seen in a variety of other spindle cell tumors
Ultrastructure
Features of fibroblastic cells
May display immature cell junctions at tips of slender cytoplasmic processes
DIFFERENTIAL DIAGNOSIS
Sarcomatoid Mesothelioma
More pronounced cytologic atypia, nuclear pleomorphism, and mitotic activity are seen in sarcomatoid mesothelioma
Diffuse, as opposed to localized, growth pattern in sarcomatoid mesothelioma
Strong cytokeratin and calretinin positivity favors sarcomatoid mesothelioma
Strong CD34, Bcl-2, and CD99 positivity favors solitary fibrous tumor
Pleural Monophasic Synovial Sarcoma
More pronounced cytologic atypia and mitotic activity are seen in synovial sarcoma
Invasive features favor synovial sarcoma over solitary fibrous tumor
Cytokeratin and EMA positivity is typically seen in synovial sarcoma but not in solitary fibrous tumor
Most synovial sarcomas are negative for CD34, but Bcl-2 and CD99 are positive in both tumors
Cytogenetic translocation (x;18) is characteristic of synovial sarcoma and is absent in solitary fibrous tumor
Peripheral Nerve Sheath Tumors
Palisading of tumor cells with Anthony type A foci are more common in schwannian tumors
S100 protein positivity is distinctive for peripheral nerve sheath tumors and is negative in solitary fibrous tumors
Both can express Bcl-2 and CD34, but CD34 is more strongly expressed in solitary fibrous tumors
Ultrastructural finding of complex, interdigitating cytoplasmic cell processes is characteristic of schwannian tumors
DIAGNOSTIC CHECKLIST
Clinically Relevant Pathologic Features
Circumscription and encapsulation
Pulmonary osteoarthropathy with clubbing of fingers
Hypoglycemia
Often found incidentally on routine chest x-rays
Pathologic Interpretation Pearls
Bland-appearing spindle cell proliferation with prominent vascular pattern and variable degrees of stromal sclerosis
Fascicular, short storiform, hemangiopericytic, neural palisading, and synovial sarcoma-like growth patterns
Variegation of histologic growth patterns within same lesion
Immunohistochemical positivity for CD34, Bcl-2, and CD99
No distinctive or pathognomonic markers available; diagnosis is by exclusion of other spindle cell tumors
So far, no known molecular or cytogenetic abnormalities
Distinction from synovial sarcoma in cellular examples of solitary fibrous tumors may require molecular studies to demonstrate t(x;18)
SELECTED REFERENCES
1. Cardillo G et al: Solitary fibrous tumors of the pleura: an analysis of 110 patients treated in a single institution. Ann Thorac Surg. 88(5):1632-7, 2009
2. Harrison-Phipps KM et al: Solitary fibrous tumors of the pleura: results of surgical treatment and long-term prognosis. J Thorac Cardiovasc Surg. 138(1):19-25, 2009
3. Kalebi AY et al: Surgically cured hypoglycemia secondary to pleural solitary fibrous tumour: case report and update review on the Doege-Potter syndrome. J Cardiothorac Surg. 4:45, 2009
4. Liu CC et al: Solitary fibrous tumors of the pleura: clinicopathological characteristics, immunohistochemical profiles, and surgical outcomes with long-term follow-up. Thorac Cardiovasc Surg. 56(5):291-7, 2008
5. Lu C et al: Solitary fibrous tumor of the pleura: an analysis of 13 cases. World J Surg. 32(8):1663-8, 2008
6. Perna V et al: Localized (solitary) fibrous tumors of the pleura: an analysis of 15 patients. Int J Surg. 6(4):298-301, 2008
7. Schirosi L et al: Pleuro-pulmonary solitary fibrous tumors: a clinicopathologic, immunohistochemical, and molecular study of 88 cases confirming the prognostic value of de Perrot staging system and p53 expression, and evaluating the role of c-kit, BRAF, PDGFRs (alpha/beta), c-met, and EGFR. Am J Surg Pathol. 32(11):1627-42, 2008
8. Chang JC et al: Hypoglycemia in a patient with a huge malignant solitary fibrous tumor of the pleura. Pathol Int. 57(12):791-3, 2007
9. Sung SH et al: Solitary fibrous tumors of the pleura: surgical outcome and clinical course. Ann Thorac Surg. 79(1):303-7, 2005
10. Bini A et al: Solitary fibrous tumor of the pleura. A single institution’s experience. J Cardiovasc Surg (Torino). 45(2):167-8, 2004
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


