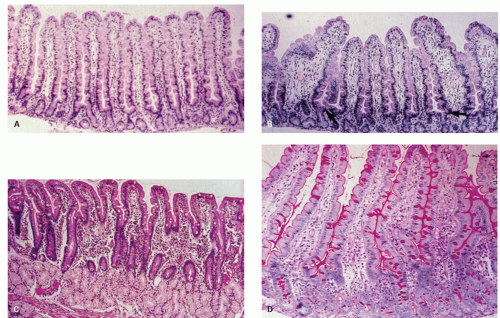
 Figure 17-1. Normal small bowel biopsy. A: Rarely are this many villi seen in a row with such perfect orientation. B: More typical appearance of a well-oriented small bowel biopsy specimen. There is some variation in villous height. The arrow points to the location of the crypt-villus junction; the villus-crypt height ratio is about 4 to 1. The bent villi at the edges of the section are broader because they are tangentially cut. C: Biopsy specimen from the duodenal bulb. The villi are normally shorter here; the crypts overlie the mucussecreting Brunner’s glands. D: Biopsy specimen stained with the PAS stain. The normal columnar cells are well visualized, and have basally oriented nuclei and a prominent brush border that is stained red-purple. The intestinal goblet cells are also well visualized and are characterized by red-purple-staining globular cytoplasm. |
anatomic variation, especially since most small bowel biopsies come from either the proximal duodenum or terminal ileum. The duodenal bulb is constantly assaulted by damaging peptic juices that often leads to Brunner gland hyperplasia, gastric surface cell metaplasia, and irregular villous architecture (see Chapter 13). The terminal ileum has numerous Peyer’s patches, which cause distortion and shortening of the villi (Fig. 17-2). Due to technical reasons, it is sometimes difficult to enter the terminal ileum resulting in biopsies that tend to be small, sometimes crushed, and frequently poorly oriented. In addition, the lamina propria is more cellular in this region. Hence, it behooves pathologists to let their endoscopists know that biopsies of the distal duodenum, proximal jejunum, or both are best for trying to diagnose malabsorptive diseases. Some villi appear more scalloped at their sides and shorter, whereas others appear more elongated and less pleated. In general, a villus to crypt ratio of 3:1 is felt to be normal.
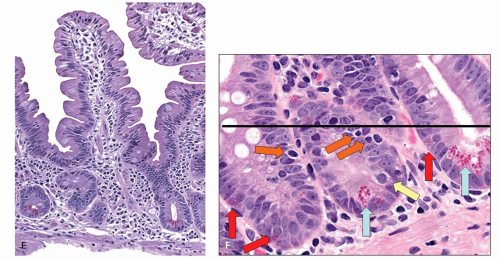 Figure 17-1. (Continued) E: Higher magnification of a normal intestinal villus showing the columnar-celled enterocytes with their basally oriented cytoplasm. F: Section of the lower half of the intestinal mucosa illustrating the intestinal crypts. Note the Paneth cells, with their characteristic red-staining granules at the base of the crypts (trichrome stain). It is important to remember that biopsy specimens fixed in Bouin’s solution rarely show Paneth cell granules, as these are dissolved by the fixative. The lamina propria between the intestinal crypts contains mononuclear cells. Plasma cells are more concentrated here than in the villous tips. |
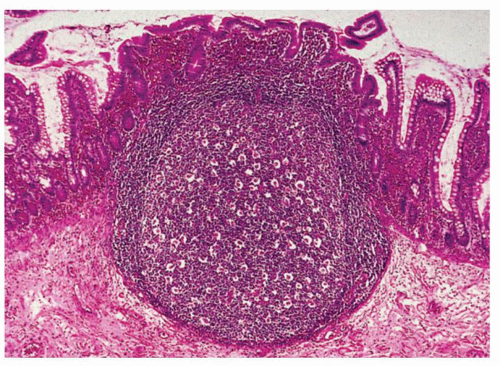 Figure 17-2. Normal small bowel mucosa overlying a hypertrophied lymphoid follicle. Note the marked blunting of the intestinal villi above the lymphoid follicle. |
branching of villi. Additionally, very shallow biopsy specimens may result in pseudoblunting (illustrated in Chapter 1). The muscularis mucosae may be absent; thus, villi appear to be stretched, separated from each other, and blunted. The clues that this appearance is an artifact and not a villous lesion are an absence of muscularis mucosae and a normal surface epithelium. In adults, villi from the duodenum are longer than ileal villi, have more indentations along their sides, and fewer goblet cells. The two can readily be distinguished by light microscopy. However, the increased numbers of goblet cells in the terminal ileum occur only over the last portion (that is the segment often biopsied), so that following ileal resections villi may look much more like proximal than distal villi.
the nuclear size is worth examining in crypt bases in case severe megaloblastic changes are present.
Table 17-1 Overview Classification of Small Bowel Biopsy | ||||||||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| ||||||||||||||||||||
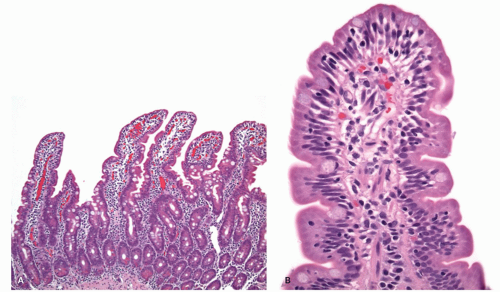 Figure 17-3. Normal villous architecture with increased intraepithelial lymphocytes (Marsh type 1). A: In this low-power view, the villous to crypt ratio is normal. B: Surface epithelium illustrates the loss of nuclear polarity and increased intraepithelial lymphocytes. |
increased cell turnover in the most common disorder associated with this lesion (i.e., celiac sprue). Biopsy specimens that are completely flat, many sometimes exhibit rudimentary villi, or villi of decreased height, all of which are encompassed by the term “partial villous atrophy.”
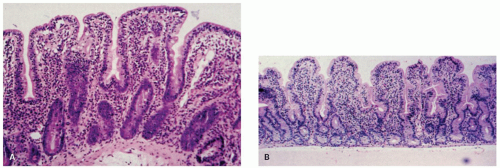 Figure 17-4. Moderate mucosal lesions (Marsh type 3b). A,B: Villi are shorter and crypts are elongated (hyperplastic), with a villus-crypt ratio of approximately 1:1. The villi are broader because of markedly increased numbers of inflammatory cells. |
be identified by their response to therapy. A few rare entities have no known treatment. In these disorders, multiple biopsy specimens from the duodenum have a diffuse, flat appearance. However, in some patients with these conditions, lesions of variable severity may be seen. A prime example is tropical sprue.
Table 17-2 Severe (Flat) Lesions: Nonspecific Histologya | ||||||||||||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| ||||||||||||||||||||||||
Table 17-3 Severe Flat Lesions: Specific/Distinctive Histology | ||||||||||
|---|---|---|---|---|---|---|---|---|---|---|
|
patients may harbor a response to avenin present in oats, besides some contamination with gluten that can be seen in commercial products.12 Gliadins can be categorized into four major fractions by gel electrophoresis, namely, alpha, beta, gamma, and omega gliadins. Early reports suggested that only the alphagliadins activated celiac sprue.13 However, subsequent studies indicate that all other components of gliadin may also activate disease.14, 15, 16 As one can imagine, defining and possibly eliminating the precise amino acid sequences of gliadin that are responsible for disease activation are topics of intense research.
Table 17-4 Variably Severe Lesions: Nonspecific Histologya | |||||||||||||||||||||||||||||||||||||||||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| |||||||||||||||||||||||||||||||||||||||||||||||||||||
Table 17-5 Variably Severe Lesions—Specific/Distinctive Histologya | |||||||||||||||||||||||||||||||||||||||||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| |||||||||||||||||||||||||||||||||||||||||||||||||||||
sprue is prevalent, but only 2% to 5% goes on to develop the disease. There is a strong familial association, with as many as 15% of asymptomatic family members having some small bowel abnormalities on biopsy, especially after a gluten challenge.18, 19, 20, 21 Celiac sprue has also been found in identical twins, but only in 70% to 75% of cases,22, 23 suggesting that additional environmental factors are important for disease expression.18, 24, 25 Such environmental factors may include viral infection. Kagnoff et al. proposed a possible role for adenovirus serotype 12 (Ad 12) in the pathogenesis of celiac sprue, based on the observation that there is a homology of amino acid sequences between a portion of alpha-gliadin and a protein (E 1b) produced by Ad 12.26 To try to confirm this, the authors looked for evidence of previous infection with Ad 12 in patients with either treated or untreated celiac sprue and in controls. They found an increased association between antibodies to Ad 12 and celiac disease in the patients compared to the controls and concluded that this finding could not be accounted for by random viral infection.27 Unfortunately, PCR studies to try and confirm the presence of Ad 12 DNA in celiac patient biopsies have been negative.28
Table 17-6 Normal Villous Architecture: Specific/Distinctive Histology | ||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
|
Variable sensitivity to gluten is also seen in patients with the disease who go off the gluten-free diet. In some there is prompt appearance of symptoms of malabsorption, whereas in others these symptoms may not reappear for months or years. The patient who presents with diarrhea may have a long-standing history of anemia or may be shorter in stature than his or her siblings. This suggests that the mucosal lesion has been present all along but that the clinical expression with diarrhea/malabsorption is delayed. Finally, it is theoretically possible that adults who present with no antecedent clues may have developed it in adulthood.
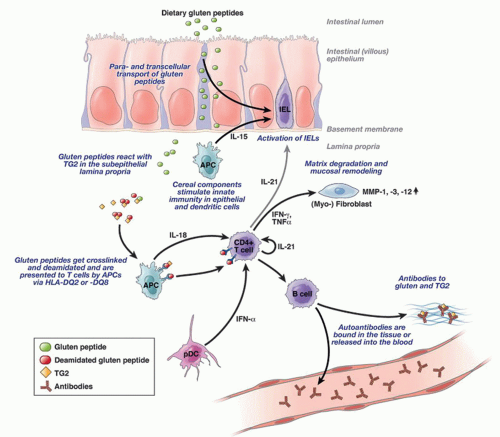 Figure 17-5. Pathogenesis of celiac disease. Gluten is transported across the epithelium by yet unclear mechanisms where crosslinking and particularly deamidation peptides in the tissue by transglutaminaase2 (TG2) creates potent immunostimulatory epitopes that are presented via HLA-DQ2 or HLA-DQ8 on antigen-presenting cells. Subsequently, CD4+ T cells are activated, secreting mainly Th1 cytokines such as IFN-γ, which induces the release and activation of metalloproteinases (MMPs) by myofibroblasts, finally resulting in mucosal remodeling and villus atrophy. Additionally, Th2 cytokines are also produced driving the production of (auto-)antibodies to gluten and TG2. Other cytokines such as IL-18, IFN-α, or IL-21 seem to play a role in polarizing and maintaining the Th1 response. The scheme is simplified. It does not show that T cells circulate to mesenteric lymph nodes where they encounter and are primed by antigen-presenting cells (mainly dendritic cells) and from where they home back to the lamina propria, a process that is driven by the lymphocyte homing receptors CCR9 and integrin α4β7. (From Schuppan D, Junker Y, Barisani D. Celiac disease: from pathogenesis to novel therapies. Gastroenterology. 2009;137(6):1912-1933.) |
1to 2 days may become much less irritable. In addition to these, the serologic tests have become equally important in establishing the diagnosis of celiac disease. TTG and antiendomysial antibodies appear to be the highly sensitive and specific serologic markers for celiac disease.34, 35 Of these, the antiendomysial antibody is considered more specific; however, it is also more expensive. Hence, in practice most often only TTG is obtained as a part of serologic testing. Some authors have advocated that following TTG titers may be a good way of monitoring a response to a glutenfree diet and thus confirming the diagnosis.45
standard for diagnosis was only histology. Nowadays, the serological testing is so robust with very positive and negative predictive values that the real clinching of a celiac disease diagnosis is made with an indicative biopsy together with positive serology. If a patient has a biopsy suggestive of celiac disease, but negative serology testing then an alternative diagnosis should be entertained. Alternatively, if a patient has positive TTG/endomysial antibody test (the most specific of the serological markers) but a completely normal duodenal biopsy then it is likely the patient has preclinical celiac disease and repeat biopsies at some time in the future may show histological changes typical of celiac disease.
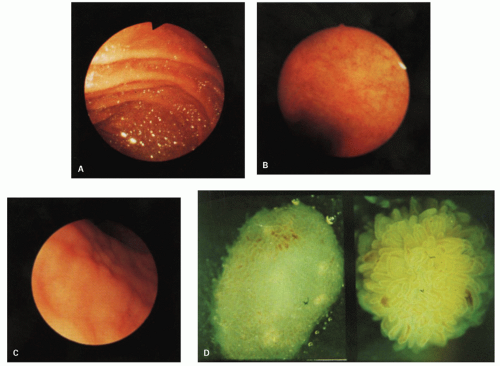 Figure 17-6. Endoscopic and dissecting microscopic appearances of the proximal small bowel in celiac sprue. A: Normal mucosal appearance with valvulae conniventes. B: Appearance in celiac sprue; valvulae are absent. C: Scalloped, ridged appearance of the mucosa on a close-up view. D: Dissecting microscopic appearance of a normal biopsy specimen (right) and a flat biopsy specimen (left). (Courtesy of Cyrus E. Rubin.) |
reconsider the diagnosis of celiac disease and worry more about either Crohn’s disease, peptic duodenitis, autoimmune enteropathy (AIE), or celiac disease, and a second disease that may be associated (e.g. Crohn’s disease) or unrelated (e.g. NSAID ingestion). Paneth cell numbers may appear reduced. It was once claimed that this might portend a suboptimal response to therapy, but this has not been confirmed. In our experience, a marked reduction in Paneth cells is rare, they may be reduced in severe lesions,66 but this does not indicate that the mucosal response will be refractory to gluten withdrawal. A complete lack of Paneth or goblet cells or both should raise the possibility of AIE. There are also reports that the numbers of certain GI endocrine cells are increased, although the clinical implications of these findings are unclear.67, 68, 69, 70
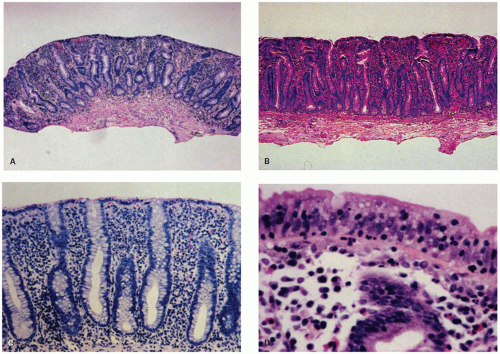 Figure 17-7. Untreated celiac sprue. Small bowel biopsy specimens showing a nonspecific severe, “flat” mucosal lesion. A,B: Lowpower views. B has an undulating surface but, at low power, is still appreciated as being flat, albeit not as flat as A. C: Medium-power magnification of superficial mucosa showing replacement of normal columnar lining epithelium by cuboidal epithelial cells. Note also the dense lymphoplasmacytic infiltrate of the lamina propria. D: High-power magnification of surface epithelium shows nuclear stratification and many small, dark-staining intraepithelial lymphocytes. |
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


