Sigmoid Colectomy: Laparoscopic Technique
Arden M. Morris
DEFINITION
Laparoscopic sigmoid colectomy is a laparoscopic procedure that involves complete or partial removal of the sigmoid colon most often with a primary anastomosis, which can be performed intra- or extracorporeally.
DIFFERENTIAL DIAGNOSIS
Laparoscopic sigmoid colectomy is most often performed to treat colon cancer or diverticulitis but may also be performed to treat a benign neoplasm, which cannot be resected endoscopically, Crohn’s or other fistulizing disease, intussusception, sigmoid volvulus, or other obstructive, inflammatory, or infectious conditions.
PATIENT HISTORY AND PHYSICAL FINDINGS
A complete history should be tailored to the patient’s primary diagnosis and should include a description of constitutional symptoms (nausea/vomiting, anorexia, weight loss or gain, fever, diaphoresis, fatigue), pain (site, quality, timing, inciting and relieving factors), dietary and bowel habits (constipation, diarrhea, frequency, continence, obstructive symptoms, bleeding), urinary habits, and sexual function.
Physical exam includes a description of the presence and quality of distension, tenderness, guarding (voluntary or involuntary), rebound, and organomegaly. It is important to check carefully for evidence of a mass. For the sigmoid colon, this should be specifically checked by using one hand to elevate the left flank and the other hand to palpate the left lower quadrant between the iliac spine and the infraumbilical midline abdomen. The presence of involuntary guarding during this maneuver may indicate inflammation of the sigmoid colon consistent with acute or smoldering diverticulitis.
A digital rectal exam must be performed preoperatively. The exam should include digital palpation of the coccyx, ischial tuberosities, and levators. The exam should include an assessment of sensation (anal wink), anal sphincter tone, and voluntary contraction (normal vs. diminished squeeze and normal relaxation vs. paradoxical puborectalis contraction with bearing down).
IMAGING AND OTHER DIAGNOSTIC STUDIES
There are many options for preoperative diagnostic imaging. For suspected diverticulitis and/or other inflammatory or fistulizing disease, abdominal/pelvis computed tomography (CT) is the most effective means for diagnosis and operative planning. In addition, CT documentation of the presence of diverticulitis is particularly important in the event that the patient’s symptoms do not abate postoperatively.
For neoplastic disease, chest/abdomen/pelvis CT should be performed to identify possible metastases to identify the extent of the tumor if possible.
Although CT with oral and rectal contrast is useful for both intra- and extraluminal assessment (FIG 1), a fluoroscopic examination with barium or water-soluble contrast enema is also useful to assess the bowel lumen especially if colonoscopy cannot be performed (FIG 2).
In the case of rectal prolapse, defecography exam preoperatively can provide additional information about the extent of sigmoid colon intussusception and the presence of an enterocele or rectocele (FIG 3).
Full colonoscopy should be performed preoperatively to assess the proximal colon and to tattoo the colon proximally and distally to neoplastic lesions (FIG 4).
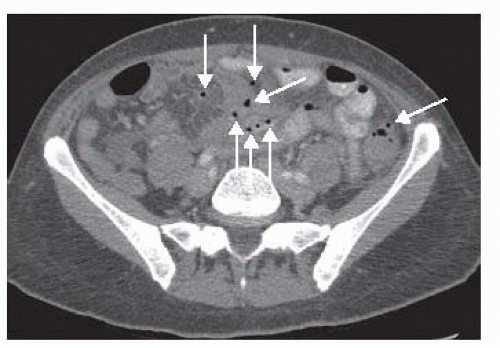 FIG 1 • Axial CT scan of the pelvis with diverticulitis and extraluminal gas (arrows). |
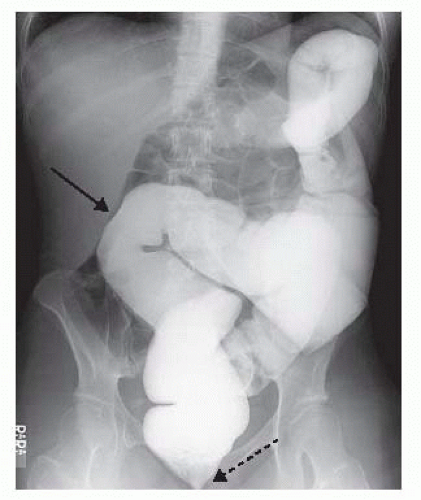 FIG 2 • Water-soluble contrast enema displaying a sigmoid volvulus (block arrow). Notice the “omega loop” configuration of the sigmoid volvulus pointing to the right upper quadrant of the abdomen and the “bird’s beak” narrowing at the entrance of the pelvis (dashed arrow). |
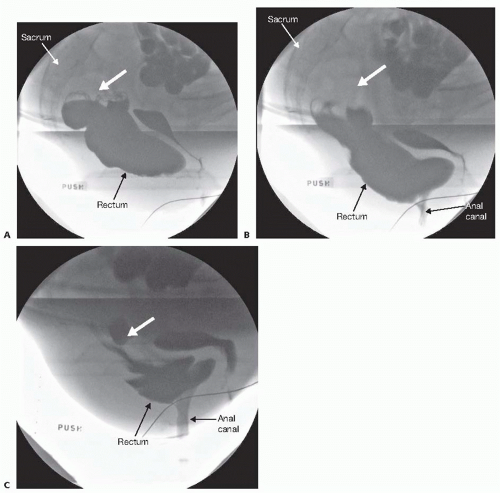 FIG 3 • A-C. Defecography displaying redundant sigmoid progressively intussuscepting into the rectum (block arrows) and thereby causing obstructed defecation. |
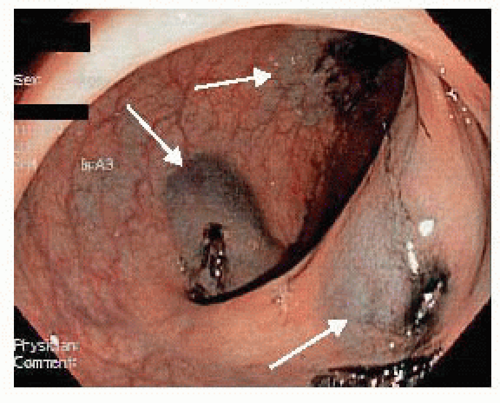 FIG 4 • Colonoscopy with submucosal injection of India ink (arrows) to mark the area of concern prior to operation. The colon is injected in three separate locations distal to the target lesion in order to maximize intraoperative localization of the target lesion. |
SURGICAL MANAGEMENT
Preoperative Planning
Although the use of a full mechanical bowel preparation continues to be debated, at a minimum the sigmoid and rectum should be cleansed of stool using enemas the night before and morning of surgery in order to drive an anastomotic stapler through the rectum for reattachment. If a complete mechanical bowel preparation is undertaken, oral antibiotics should be included.
Although use of laparoscopy has reduced risk of wound infections among patients undergoing colon surgery, risk of deep-space organ infections remains. Broad-spectrum intravenous antibiotics should be given within 30 minutes prior to the abdominal incision. Intraoperatively, antibiotic redosing should be discussed by the surgeon and anesthesiologist for any operation that lasts 4 hours or longer.
Risk of deep venous thrombosis is increased among patients with a diagnosis or cancer or inflammatory bowel disease, patients who undergo abdominal or pelvic surgery, and those who have prolonged operations. Patients who undergo laparoscopic sigmoid colectomy fulfill several of these criteria and therefore are at substantially increased risk of venous thrombosis. To reduce this risk, sequential compression devices should be applied to bilateral lower extremities and initiated preinduction, when they are most effective at countering the effects of periinduction venous pooling. After induction, 5,000 units of heparin should be delivered subcutaneously.
Patient Positioning
After endotracheal general anesthesia has been induced, the patient is placed in a split-leg or dorsal lithotomy position and secured in a beanbag, with careful attention to padding the extremities, tucking the right arm at the side, and lowering the thighs to be parallel to the floor if possible. If the hips are flexed, the thighs are higher than the abdomen and can hinder the laparoscopic dissection (FIG 5).
Tape the patient across the chest over a towel to secure him or her to the operating room (OR) table.
A urinary catheter is placed to decompress the bladder and assist with monitoring urine output during the operation. If the normal anatomic location of the left ureter has been compromised by previous surgery or by an inflammatory condition such as diverticulitis, which can shorten the mesentery and pull the ureter medially, then placement of a ureteral stent or a lighted ureteral stent should be considered.
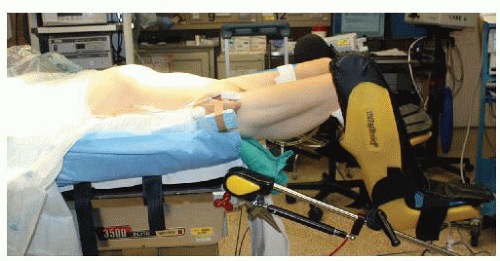
FIG 5 • Patient positioning. The patient is placed on a low lithotomy position with the legs on Yellofin stirrups. The thighs are positioned parallel to the ground to avoid conflict with the surgeon’s arms. The patient is placed on a beanbag with both arms tucked and taped to the table over a towel. All pressure points are padded to prevent neurovascular injuries.
An orogastric tube is placed to decompress the stomach.
If the mechanical bowel preparation or preoperative enemas are inadequate, the surgeon should perform a rigid sigmoidoscopy to clear the rectum of stool after endotracheal general anesthesia has been induced.
Most hospitals in the United States now require a robust time-out that includes a verbal statement of the patient’s identification, diagnosis, medications and allergies, the planned procedure, and positioning, as well as the names and roles of the operating team and a list of necessary equipment and potential problems.
TECHNIQUES
PORT PLACEMENT AND OPERATING TEAM SETUP
The surgeon stands to the patient’s right side, with the scrub nurse next to him or her. The assistant stands to the left side of the table (FIG 6). Two monitors, facing the surgeon and the assistant, are used.
A 12-mm umbilical incision is created sharply and extended to the level of the fascia. The fascia is elevated with 2-0 Vicryl tacking sutures and then opened sharply. The Hasson port is then placed within the peritoneal cavity and tacking sutures are pulled up and clamped. This will be used as the camera port.
Insufflation with carbon dioxide (CO2) at high flow is initiated to an appropriate pressure of approximately 14 mmHg.
After inspection of the abdominal cavity with the laparoscope, three additional 5-mm working ports are placed under visualization in the right upper, right lower, and left lower quadrants of the abdomen (FIG 7).
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


