Shaping Genetic Policy: The United States Initiatives
Shaping Genetic Policy: The United States Initiatives
Agnes Masny MSN, MPH, RN, CRNP
Introduction
With the completion of the Human Genome Project we now have a better understanding of the molecular cause and modification of specific diseases or conditions. Genetic technologies that accompany these discoveries are helping to predict who may be at risk for disease, to analyze gene interactions that modify disease, to establish clinical guidelines for diagnoses and prognoses of disease, to identify genes associated with diseases, and to screen newborns for disease. These new discoveries and technologies promise to provide genetic information about our family, our society, changing the life of every United States citizen. But how will these discoveries reach every American? How will they come to be used for good and not harm? Public health policy shapes the answer to this question.
Genetics Policy Development in the Context of Health Policy
Any new health discovery carries with it the potential of good or harm to the individual or society. Government oversight helps provide direction to influence legislation or judicial action that affects the allocation or regulation of specific goods to achieve benefits for society (Longest 2002). Strictly speaking, appropriate allocation and regulation of resources is the goal of all public health policy. The completion of the Human Genome Project and the multitude of genetic and genomic discoveries following the sequencing of the human genome have driven current health policy regarding genetics. This, in turn, has created public demand for genetic technologies and services and subsequent public concern about privacy, discrimination, access, stigmatization, and misuse of genetic information. Therefore genetic health policy must address the scientific and ethical challenges of genetic testing and technologies.
Policy in the United States is determined by the interaction of the executive, judicial and legislative branches of government and the public reaction to laws and policy. Public concern and civil suits may help to initiate a policy response at the executive or legislative level, such as the protections for the disabled provided by the Americans with Disabilities Act (ADA) of 1990. Or the accumulation of legal cases may draw attention to the need for legislative protections at the state or federal level. In 1996, the Health Insurance Portability and Accountability Act (HIPAA) was a legislative response to employees’ concerns about losing health insurance after changing jobs or becoming unemployed.
Another approach to policy development is executive oversight of issues that affect the public. The Department of Health and Human Services (DHHS), one of the 15 executive departments, provides protection for the health and welfare of all Americans and access to essential human services. Although these departments fall under the executive branch of government, they influence legislation, policy, and national guidelines. Specifically, DHHS is responsible for many of the regulatory, programmatic, and financial aspects of the healthcare system and plays a key role in the planning, delivery, and financing of health care. DHHS programs are administered by 11 operating divisions, including 8 agencies in the Public Health Service and 3 human service agencies (agencies and divisions are listed online at http://www. hhs.gov/about/whatwedo.html/).
One of the roles of the executive departments is to advise the president on current policy and legislative actions, policy research, evaluation, and economic analysis of issues that the department oversees. Additionally, Public Law 92-463 of the Public Health Services Act provides for department heads to form and use advisory committees. This executive approach to policy formation has been widely used to address genetic issues. DHHS has provided a forum for expert discussion and public review of genetic issues through two of its advisory committees, the Secretary’s Advisory Committee on Genetic Testing (SACGT), convened from 1998 to 2002, and the Secretary’s Advisory Committee on Genetics Health and Society (SACGHS), convened in 2002 and actively meeting at this printing. Recommendations from these advisory committees have also helped to guide the secretary of DHHS in making policy recommendations (see Table 3-1).
Program of the Human Genome Project to study ethical and social issues emerging from use of genetic information.
1995
Task Force on Genetic Testing
Charged by ELSI to make recommendations for safe and effective genetic tests.
1998
Secretary’s Advisory Committee on Genetic Testing (SACGT)
Recommended by Task Force on Genetic Testing and chartered by Secretary of Health and Human Services (HHS) Donna Shalala to develop oversight measures for safe and effective genetic testing.
Secretary’s Advisory Committee on Genetics, Health and Society (SACGHS)
Chartered by HHS Secretary Tommy Thompson for two years to study and advise secretary on broad range of genetic and genomic applications in health care and society.
Ethical Considerations Regarding Genetics Prompts Government Response
Ethical concerns were recognized early as a potential impact of the Human Genome Project. These issues included confidentiality, genetic test accuracy, the burden of genetic knowledge for the individual, and the misuse of genetic information leading to discrimination or stigmatization. (Botkin 1990; Juengst 1997/1998). The Department of Energy (DOE) and the National Institutes of Health (NIH) also recognized these concerns and devoted 5% of the Human Genome Project budget to study the ethical, legal, and social issues arising from clinical use of genetic information. The Ethical, Legal and Social Issues (ELSI) program identified several topics for study and oversight, including how genetic information would be used, how genetic information affects members of a family or a community, privacy, confidentiality, patenting, access to personal sequence data by insurance companies, potential for job discrimination based on personal sequence data, and the prospects for genetic screening, therapy, and engineering.
In 1995, the Committee to Evaluate the Ethical, Legal and Social Implications Program of the Human Genome Project was charged with reviewing the work of the Joint NIH and DOE working group of ELSI. In turn, the committee charged a Task Force on Genetic Testing to review genetic testing in the United States and to make recommendations to ensure the development of safe and effective genetic tests. In its final report the Task Force on Genetic Testing identified four major areas of concern: “(1) the way in which tests are introduced into clinical practice; (2) the adequacy and appropriate regulation of laboratory quality assurance; (3) the understanding of genetics on the part of healthcare providers and patients; and (4) the continued availability and quality of testing for rare diseases” (NHGRI 1997). Although the task force recommended the establishment of a process for genetic test development and review, it did not specify changes in existing laboratory reviews to incorporate new genetic tests (Holtzman 1999). Thus, the formation of an advisory committee to the secretary of DHHS was recommended by the NIH–DOE Task Force on Genetic Testing and the Joint NIH–DOE Committee to evaluate the ELSI program of the Human Genome Project. These groups pointed out the need for public policy development in helping national leaders deal with the benefits and challenges of genetic testing and its corresponding information.
Secretary’s Advisory Committee on Genetic Testing (SACGT)
Responding to the joint recommendations of the Task Force on Genetic Testing and the NIH–DOE committee, DHHS, under the directorship of Secretary of Health and Human Services Donna Shalala, chartered the SACGT in June of 1998. DHHS requested that SACGT build on the work of the task force to assess whether current programs for ensuring the accuracy and effectiveness of genetic tests were satisfactory. This assessment required consideration of the potential benefits and risks (including socioeconomic, psychological, and medical harms) to individuals, families, and society. If, after assessment and public consultation, further measures were deemed necessary, SACGT was further charged to recommend oversight measures for genetic tests.
SACGT was primarily charged with assessing oversight of genetic tests, but the training and education of healthcare providers and the promotion of greater public understanding of genetics were also key areas for policy consideration. Public consultation was a key strategy for SACGT; genetic public policy needed the input of a wide range of stakeholders. Therefore, attempts to gather public input included requests for public comment in the Federal Register, mailings to professional organizations, opportunities to provide public comments during meetings, and specially convened public meetings to gather the public’s perspective on genetic testing limitations, benefits and risks, and the accessibility of genetic tests to diverse populations (SACGT 1999).
Secretary’s Advisory Committee on Genetics Health and Society (SACGHS)
With a change in administration in 2002, the SACGT was disbanded. In September 2002, Secretary of Health and Human Services Tommy Thompson chartered a new advisory committee to continue the discussion and deliberations on the ethical and social issues raised by advances in genetics. SACGHS was charged with a range of functions including:
assessing how genetic technologies are integrated into health care and public health; studying the clinical, ethical, legal, and societal implications of genetic applications, such as pre-implantation diagnosis and emerging technological approaches to clinical testing; identifying opportunities and gaps in research and data collection efforts; exploring the use of bioterrorism; examining patent policy and licensing practices for their impact on access to genetics technologies; analyzing uses of genetic information in education, employment, insurance, including health disability, long-term care, and life, and law, including family, immigration, and forensics; and serving as a public forum for discussion of emerging scientific, ethical, legal, and social issues raised by genetic technologies. (DHHS 2002)
Early deliberations of SACGHS recognized that the scope of the committee’s work included both genetics and genomics. Whereas genetics focuses one or a few germlines—inherited or acquired mutations in the genome associated with a specific diseases or conditions—genomics focuses on a large number of genes in the genome as they interact with endogenous and exogenous factors impacting health and disease (SACGHS 2006; Guttmacher, Collins, and Drazen 2004). Discussions and recommendations of SACGHS regarding genetic tests and services were expressly intended to cover future uses of genetic and genomic technologies.
Initially health professionals objected that attention to recommendations already made from the SACGT would be diluted or lost in the broad range of issues proposed for SACGHS (Michaels, Bingham, Boden, Clapp, Goldman, Hoppin, et al. 2002). However, SACGHS has tried to incorporate the previous work and advice of SACGT into its own. Furthermore, SACGHS has made attempts to identify critical issues. Early meetings included informational presentations designed to provide the committee with an understanding of the issues encompassed in its charter and the background needed to identify and prioritize issues. For example, leading experts reviewed existing and emerging directions in genetic technologies and their clinical and public health applications; the financing of genetic technologies in the U.S. healthcare system; and future directions in genetics and genomics research, to name a few. After hearing from experts SACGHS appointed an advisory committee to design a prioritization process, by which they arrived at twelve genetic/genomic technologies and services:
Access
Coverage and reimbursement
Direct-to-consumer marketing
Genetic discrimination
Genetic education and training
Genetic exceptionalism (treating genetic information as distinct from medical information and requiring special consideration)
Large population studies
Oversight of genetic testing
Patents and access
Pharmacogenomics
Public awareness
Vision statement
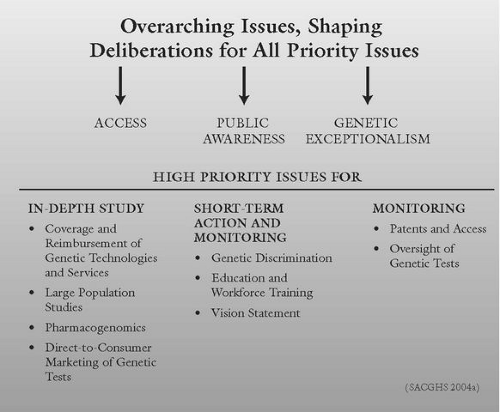
The committee organized the priority issues into four categories (see Figure 3-1):
High-priority issues that warrant more in-depth study,
High-priority issues that can be addressed in a relatively straightforward way or with short-term action plans,
High-priority issues requiring only monitoring, and
Overarching issues that should be considered within the context of deliberations and recommendations for all issues.
FIGURE 3-1SACGHS Categories of Genetics/Genomics Priority Issues in Health Care
The priority issues and their policy considerations, with the exception of public awareness and the vision statement, are discussed below. These priority issues are abridged from A Roadmap for the Integration of Genetics and Genomics into Health and Society (SACGHS 2004a) and can be viewed in their entirety online. The issues of public awareness and a vision statement pertain to all the other priority areas, but by themselves do not raise specific ethical concerns.
Access to Genetic Technologies
Barriers to the accessibility of genetic technologies can prevent patients and consumers from fully benefiting from genetic services and advances in genetics. Both SACGT and SACGHS recognized the importance of populations having access to genetic research and technologies. The cost of genetic testing and services as well as insurance coverage were identified as potential barriers to access.
Policy Considerations
The federal government places a high priority on access to health care.
Many issues in genetics have an access component. Access provides a context to consider all priority issues.
Barriers to and disparities in access are issues endemic to the entire healthcare system, and because genetics is integrated in numerous medical disciplines, efforts to address specific aspects of access throughout the healthcare system may be difficult and better addressed by a legislative body with a broader mandate.
Policy Efforts
Several SACGT efforts were directed to explore the financial barriers to access as well as disparities in access to genetic testing services. SACGT formed an Access Working Group and contributed to a Coverage and Reimbursement Issue Brief. The work group also held a town meeting on disparities in access to genetic testing. Since SACGHS identified access to genetic technologies as an overarching issue, this priority issue became a recurrent theme for all the other issues. Further details on SACGT‘s and SACGHS‘s efforts are found under “Coverage and Reimbursement.”
Coverage and Reimbursement of Genetic Technologies
Decisions made by public and private health plans about coverage and reimbursement influence the quality and cost of health care. Coverage and reimbursement also influences individuals’ access to providers, services, procedures, and tests. Eighty-five percent of Americans have some health insurance through individual, employer-based plans or public insurance programs such as Medicare and Medicaid. Therefore, health insurance coverage and reimbursement to genetic technologies is a key factor in access to services and health outcomes.
For the most part, coverage decisions, including those for genetic technologies, are made by private insurers on a case-by-case basis or by a formal coverage policy that is applicable to all plan holders. Most formal policies include criteria for coverage, such as the presence of evidence-based risk factors (e.g., symptoms, family history) or that the results will influence treatment decisions.
Policy Considerations
Medicare payments are important, as they establish the upper limit of what Medicaid can pay for the same service and may provide the basis on which private healthcare payers determine payment amounts.
By law, Medicare cannot cover screening tests done in the absence of signs, symptoms, or personal history of disease.
Most health plans provide coverage for preventive service. Genetic tests, on the other hand, are not generally covered.
The Clinical Laboratory Fee Schedule is established by the Centers for Medicare and Medicaid Services (CMS) and determines Medicare’s payment amounts for laboratory tests including genetic tests.
Because the U.S. healthcare financing system is complex and involves numerous stakeholders, recommendations on coverage and reimbursement need to target all sectors: federal agencies and programs (e.g., CMS/Medicare, Agency for Healthcare Research and Quality, Health Resources and Services Administration, Federal Employee Health Benefit Plan, military health plan), state agencies and programs (e.g., Medicaid), and the private and professional sectors.
Recommendations aimed at federal programs may be effective based on SACGHS‘s placement within DHHS and its advisory role to the secretary of DHHS.
Only gold members can continue reading. Log In or Register to continue