School Age and Adolescence
In certain cultural and religious groups, the age of 7 years is a significant developmental milestone. The Catholic Church considers children of this age to have attained the ability to reason and thus designates it the age for the First Holy Communion. Formal schooling, the development of conscience and morality, and the ability to function in the world independent from the family, all start at about this age.
The age of 20 years is another significant development milestone. Childhood is over, adolescence is coming to an end, and the individual must now be physically and socially prepared to face the challenges and enjoy the privileges of adult life.
• SCHOOL AGE: 7 TO 11 YEARS
Compared with earlier and later ages, the schoolage years of 7 to 11 are a relatively carefree time for children. Many difficult physical and psychological tasks have been mastered, and psychosexual issues are dormant. The child can now refine her motor, social, and intellectual skills and, as an independent person, experience the outside world of peers and new experiences. Erikson, describing this stage as industry versus inferiority, said that development of these skills with hard work (i.e., industry) can lead to a lifelong sense of competence. In contrast, failure to achieve these goals can result in persistent feelings of low self-esteem.
School and learning
As in most modern societies, formal schooling in the United States begins at about the age of 7 years. At this age, children acquire the capacity for logical thought. Piaget noted that it was necessary to have this skill to be able to reason and learn mathematical concepts, and he called this developmental period the stage of concrete operations. For example, a child with concrete operational skills can understand that objects can have more than one property—a toy can be both red and metal—and that the quantity of any substance remains the same regardless of the size of the container it is in. Piaget called the latter concept the concept of conservation. For example, the 7-year-old child, but not the 4-year-old child, can understand that two containers contain the same amount of water even though one is a tall, thin tube and the other is a short, wide bowl (Fig. 2-1). Because of the speed at which these abilities must be gained, previously unidentified learning problems often become obvious at the start of formal schooling.
Play and peer relationships
The social life of school-age children revolves around school, as well as sports and other extramural activities. It is through these pursuits that children gain a sense of mastery and self-esteem and begin to form social relationships with adults who are not their caregivers. Teachers, sports coaches, and scout leaders become supplemental role models, and their approval and support grow in importance to the child. Children also develop a sense of competence through the pursuit of hobbies. Here they can use their newly acquired organizational skills to catalog and track collections of objects, such as stamps, coins, dolls, or trading cards.
Peer relationships, particularly with children of the same sex, also increase in importance during the school-age years. Children of this age typically have a small group of friends with whom they communicate, often about their similarities in attitudes and beliefs and the dissimilarities of children outside the group. Popular children typically have good interpersonal skills and follow the rules. Children who do not “fit in” and are rejected by the group commonly fall into one of two types: those who are depressed, anxious, and have low self-esteem, and those who are overly aggressive or “bossy.” Exercises aimed at helping unpopular children learn and practice social skills can help them make new friendships. Also, because these children typically have poor attitudes toward school, such interventions have the added benefit of improving school performance.
Sexuality
With the sexual and romantic feelings of adolescence yet to come, the quiescent sexuality that
characterizes the 7- to 11-year age group led Freud to describe this developmental period as latency. The latency-age child typically identifies himself or herself with the parent or caregiver of the same sex and wants to be just like that person when he or she grows up. Children of this age also have little social interest in those of the opposite sex. Boys prefer to play with boys and girls with girls. They may even describe children of the opposite sex as “silly” or “yucky.” This attitude will change dramatically in just a few years.
characterizes the 7- to 11-year age group led Freud to describe this developmental period as latency. The latency-age child typically identifies himself or herself with the parent or caregiver of the same sex and wants to be just like that person when he or she grows up. Children of this age also have little social interest in those of the opposite sex. Boys prefer to play with boys and girls with girls. They may even describe children of the opposite sex as “silly” or “yucky.” This attitude will change dramatically in just a few years.
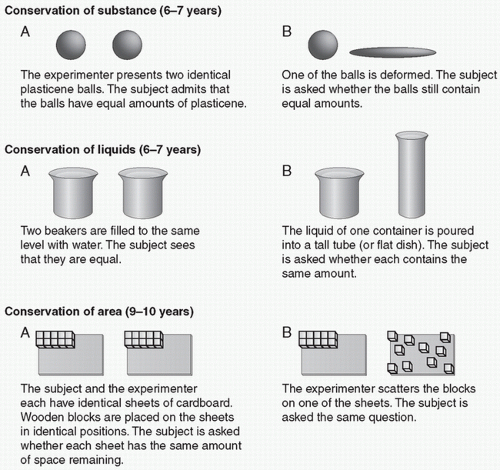 FIGURE 2-1. Tests evaluating the concept of conservation. (Reprinted with permission from Lefrançois, G. (2001). Of children: An introduction to child and adolescent development (9th ed.). Belmont, CA: Wadsworth Publishing.) |
The development of morality
In contrast to younger children, who are almost totally self-involved (see Chapter 1), 6- to 7-year-old children have begun to develop the ability to put themselves in another person’s position and to internalize a sense of right and wrong. Development of these feelings of empathy and morality continues throughout the school years.
In the first stages of the transition from selfinvolvement to understanding others, and like a convert to a new religion, the child has more of an awareness of right and wrong and is more rule-conscious than an older child or adult. The 7-year-old insists that the Monopoly board game be played strictly by the rules; no player “gets out of jail” until he gives up three turns. Later, as the child begins to understand another person’s point of view, he becomes more accepting and flexible in social interactions. The 12-year-old can bend the rules and allow players who are losing to leave jail and resume the game after only one missing turn.
Maturation of the nervous system permits the latency-age child to engage in complex motor tasks. This, coupled with the child’s growing internal sense of morality, results in her interest in and ability to follow the often complex rules of team sports.
Illness
Compared with younger or older children, schoolage children cope well with illness and hospitalization. Thus, when there is a choice, this is the best age to perform elective surgery. Although most cope
well, some school-age children (and adolescents) who are ill or who have an ill sibling or parent may respond by misbehaving at school or home (i.e., using the defense mechanism of acting out [see Chapter 8]). Others may become anxious, depressed, or withdrawn.
well, some school-age children (and adolescents) who are ill or who have an ill sibling or parent may respond by misbehaving at school or home (i.e., using the defense mechanism of acting out [see Chapter 8]). Others may become anxious, depressed, or withdrawn.
Another important milestone of this age is comprehending the finality of death. As discussed in Chapter 1, the 6-year-old child begins to understand that death is final and fears that his parents will die and leave him. At about the age of 9 years, the child begins to understand that children also can die and he may begin to fear his own death. If a child is in fact seriously or even terminally ill, the question of whether, when, and how to tell him about the prognosis is a difficult one for parents and physicians (see Chapter 24).
• ADOLESCENCE: 11 TO 20 YEARS
For convenience, adolescence can be divided into early (ages 11 to 14 years), middle (ages 15 to 17 years), and late (ages 18 to 20 years) phases. All three phases are characterized by the further development of independence and autonomy as well as the new requirements of personal decision making.
Changes in the brain associated with adolescence include continuation of the myelination that began earlier in development leading to increased white matter to gray matter volume. This increase is particularly noticeable in the frontal and parietal lobes and is positively correlated with the adolescent’s improved cognitive abilities. Another change in the brain at this time is the pruning of up to 50% of the synaptic connections made exuberantly during childhood as well as a decline in glucose and oxygen metabolism.
table 2.1 TANNER STAGES OF SEXUAL DEVELOPMENT | ||||||||||||||||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| ||||||||||||||||||||||||||||
Early adolescence (11 to 14 years)
Puberty is the physical indicator of the start of adolescence. This milestone is marked by increased skeletal growth and the development of primary and secondary sex characteristics. Girls reach puberty earlier than boys. In the United States, the average age of the start of pubertal development is 10.5 years in girls (normal range 8.0 to 13.5 years) and 11.5 years in boys (normal range 9.5 to 13.5 years). First menstruation, or menarche, usually occurs between 11 and 14 years, and first ejaculation, a marker of puberty in boys, occurs between 12 and 15 years. The physical process of puberty is usually complete by an average age of 13.5 years in girls and 15.0 years in boys, with normal ranges of 10.5 to 17.0 and 13.5 to 17.0 in girls and boys, respectively. Tanner staging classifies puberty into five levels—from immature, Stage 1 to mature, Stage 5 based on the development of secondary sex characteristics (Table 2-1).
The remarkable physical changes of adolescence, coupled with a teenager’s increased concern about physical appearance, can render any alteration in the expected pattern of development such as
acne, obesity, or late breast development, particularly stressful.
acne, obesity, or late breast development, particularly stressful.
Although sensitive to the opinions of peers, early adolescents usually are obedient (unlike older teens) and are unlikely to seriously oppose parental authority.
Middle adolescence
By about age 15 years, the adolescent has a great interest in body image and in popularity with same- and opposite-sex peers. To fit in with peers, the middle adolescent embraces current fashions in clothing and music and prefers to spend time with friends rather than family. This behavior is expected and normal, but it can lead to conflict with parents.
In part because of a readiness to challenge the rules and feelings of invulnerability, the middle adolescent is also more likely than younger or older adolescents to engage in risk-taking behavior. This behavior can take the form of failure to use birth control, smoking cigarettes, and taking drugs, and can thus have potentially serious medical consequences. Warning an adolescent of the long-term consequences of her risk-taking behavior has limited effectiveness. Education about obvious short-term benefits, particularly on physical appearance or popularity, is more likely to decrease a teenager’s unwanted behavior. For example, pointing out that smoking will darken her teeth or cause bad breath is more likely to influence a teenager’s smoking behavior than telling her that she is at increased, long-term risk for lung cancer.
Because they may lose, albeit temporarily, their valued, newly acquired autonomy and need for privacy, medically ill middle adolescents may be reluctant to comply with medical advice. This reaction can challenge the patience of parents and even the most dedicated doctor.
Late adolescence (18 to 20 years)
Late adolescence is associated with an identity crisis, in which the teen must define and refine his place in the world. Resolution of this crisis usually results in the further development of morals, ethics, and self-control, as well as the ability to realistically appraise one’s own abilities. In most countries, this age group (usually college students) becomes vocal about humanitarian issues and world problems and initiates protest movements for social change. Erikson said that adolescents who have difficulty forming their identities and finding their places in the world demonstrate role confusion. With role confusion, the teen may display behavioral abnormalities, such as criminality, drug abuse, or an interest in cults.
As for learning, some, but not all, late adolescents develop the ability for abstract, hypothetical, or formal reasoning like that required for calculus. Piaget called this stage of cognitive development formal operations.
Teenage sexuality and pregnancy
Adolescence is marked not only by cognitive maturation and personality formation, but also by strong sexual feelings. These feelings are expressed through physical activity and through masturbation. Daily masturbation throughout adolescence (and later) is a normal occurrence, and heterosexual or homosexual crushes—feelings of love for an unattainable person such as a rock star—are common. Homosexual experiences may occur during adolescence and may or may not be initial expressions of a homosexual orientation. And, although parents may become alarmed, such practicing is part of normal development.
In the United States, the average age of first sexual intercourse is about 16 years. By 19 years of age, most men and women have had intercourse. Because the average age of first marriage is about 23 years, sex before marriage is the norm in this society.
Fewer than half of all sexually active teenagers regularly use contraceptives. The reasons for this are varied, but teenagers are often convinced that they are “special” and “different” and thus will not get pregnant or develop a sexually transmitted disease (STD). This conviction is not based on fact. In 2000, the 15- to 19-year-old age group had the highest age-specific gonorrhea rate among women (716 cases per 100,000) and the third highest rate among men (328 cases per 100,000). Chlamydia, one of the most common STDs, is more common in adolescent women than in older women. Other reasons for failure of teens to use contraceptives include lack of access to them or not knowing which methods are effective.
Emotional and social factors that predispose teens to pregnancy include depression, poor school achievement, and divorced parents. Although the pregnancy rate in American teenagers is currently decreasing, about one-third of American girls get pregnant before the age of 20. In contrast, the pregnancy rate among older women, particularly those over age 40 years, is increasing (Fig. 2-2). Pregnant teenagers can present a challenge to physicians because they are at higher risk for obstetric complications than older patients. This is true in part because teens are less likely to seek prenatal care than older patients and also because they are physically immature.
Most medical care to minors (those under age 18 years) requires parental consent. However, it is usually both ethical and legal for physicians to
provide minors with sexual counseling and contraceptives without parental knowledge or consent, as well as provide treatment for STDs, problems associated with pregnancy, and drug and alcohol abuse (see Chapter 26).
provide minors with sexual counseling and contraceptives without parental knowledge or consent, as well as provide treatment for STDs, problems associated with pregnancy, and drug and alcohol abuse (see Chapter 26).
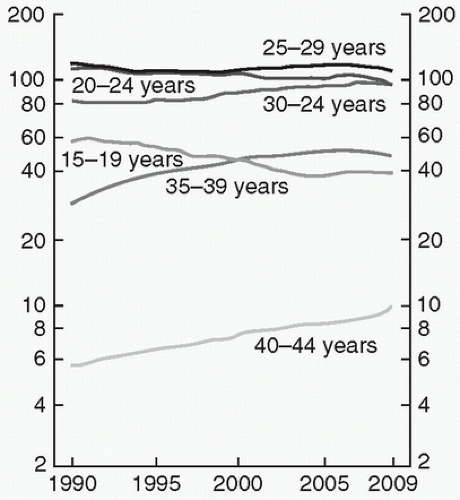 FIGURE 2-2. Birth rates in the United States by age of mother: 1990 to 2008 and preliminary 2009 (Reprinted from Hamilton, B. E., Martin, J. A., Ventura S. J., & Division of Vital Statistics. (2009). Births: Preliminary data for 2009. Nat Vital Stat Rep, 5,3 9(3),3.) NOTE: Rates are plotted on a logarithmic scale. SOURCE: CDC/NCHS, National Vital Statistics System. |
The Supreme Court decision of Roe versus Wade in 1973 made first-trimester abortion




Stay updated, free articles. Join our Telegram channel
Full access? Get Clinical Tree
