Restorative Proctocolectomy: Single-Incision Laparoscopic Technique (Including Pouch Ileoanal Anastomosis)
Theodoros Voloyiannis
DEFINITION
Single-incision laparoscopic restorative proctocolectomy, including pouch ileoanal anastomosis with temporary diverting loop ileostomy, is another application of the single-incision laparoscopic technique where a single multichannel laparoscopic port is used via a 2.5- to 3.5-cm total incision length.
The procedure can be performed for benign or neoplastic diseases that require elective restorative proctocolectomy with a hand-sewn or stapled coloanal anastomosis including ileoanal pouch anastomosis such as ulcerative pancolitis, polyposis syndromes such as familial adenomatous polyposis or synchronous noninvasive rectal carcinoma and colonic carcinomas and polyps after appropriate oncologic staging workup.
A variation of this procedure may be applied for mid- or low rectal cancer with adequate oncologic distal rectal wall margin, preferably of at least 2 cm, for creation of an anastomosis. In these cases, a low anterior resection with stapled coloproctostomy or hand-sewn coloanal anastomosis and temporary loop ileostomy may be performed.
A completion proctectomy, an ileoanal pouch anastomosis with temporary loop ileostomy after a total abdominal colectomy for ulcerative colitis, is another application of this technique.
A new approach, the transabdominal-transanal single-port technique or transanal single-port total mesorectal excision (ta-TME) for completion of the total mesorectal excision with placement of a transanal single port, is discussed in this chapter.
The goal is to keep the procedure simple, safe, and cost effective, with comparable outcomes to hand-assisted or multiport laparoscopic technique.
Although single-incision laparoscopic surgery differs technically from conventional laparoscopic surgery, it follows the same steps and oncologic principles. However, it requires advanced laparoscopic skills.
PATIENT HISTORY AND PHYSICAL FINDINGS
A detailed history and physical examination is essential preoperatively to determine if the patient is suitable for a laparoscopic approach. Rectal neoplasia after preoperative neoadjuvant chemoradiation or T4 rectal tumor extension to the sacrum, bladder trigone, prostate, posterior vaginal wall, or side pelvic wall with ureteral or major vessel involvement should be addressed preoperatively with appropriate staging workup. In these cases, laparotomy may be the best option, or if the procedure can be accomplished laparoscopically, a hybrid approach with a single-port laparoscopic technique at the suprapubic area with subsequent conversion to a Pfannenstiel incision may be considered.
Potential intraoperative consultation to other subspecialties, such as gynecology for addressing an incidental neoplastic adnexal pathology, urology for ureteral or bladder tumor involvement or other surgical service, may be necessary. It is the primary surgeon’s responsibility to communicate with the consulting service regarding the feasibility of a singleincision laparoscopic approach in order to avoid a lengthy single-incision procedure that may lead to conversion to hand-assisted laparoscopy or to a laparotomy.
A restorative proctocolectomy allows for extraction of the specimen via the single port or transanally, in case of a planned coloanal or ileoanal pouch hand-sewn anastomosis. A full-thickness rectal division is performed at the level of the dentate line. In case of underlying colonic or rectal neoplasia, the size of the tumor determines if it can be extracted without tension via the single-port wound protector. In general, tumors up to 7 cm can be extracted via a 5-cm maximum length single incision. The procedure can still be performed with elongation of the incision for extraction of larger tumors. In that case, the benefit of the single port is eliminated, with the exception of the avoidance of use of multiple laparoscopic ports. If the single port is placed via the new ileostomy site, then partial approximation of the fascia may be required prior to maturation of the ileostomy.
A large palpable tumor preoperatively with fixation to the abdominal wall or other organs may be a contraindication to single-incision laparoscopy, although excision en bloc with soft tissue abdominal wall is still possible via a single incision in some cases.
It is important to define the underlying pathology—benign versus malignant disease and the location of the lesion—preoperatively. Neoplasia may require formal lymphadenectomy with preferable high ligation of the involved vascular supply. This may not be necessary in benign conditions such as ulcerative colitis or polyposis syndromes without dysplasia or neoplasia.
In case of a planned ileoanal pouch anastomosis, particular attention is paid to the preservation of the ileocolic vascular pedicle in order to maintain the vascular supply of the pouch. The ileal pouch can be fashioned extracorporeally, following extraction of the colon and rectum via the single incision wound protector.
Previous abdominal surgeries with extensive abdominal or pelvic adhesions may increase the operative time.
IMAGING AND OTHER DIAGNOSTIC STUDIES
Preoperative colonoscopy is necessary to justify the planned restorative proctocolectomy.
Diagnosis of ulcerative colitis and exclusion of Crohn’s disease by colonoscopic biopsy and by an experienced pathologist
and/or with the assistance of other laboratory workup, such as Prometheus test, are necessary in order to establish the need for restorative proctocolectomy with ileoanal anastomosis.
Colonoscopic evidence of terminal ileitis by biopsy may assist in the diagnosis of Crohn’s disease and avoidance of an ileoanal pouch formation.
Diagnosis of ulcerative colitis with proctitis and involvement of the anal canal by colonoscopy or rigid proctoscopy and biopsy is necessary in order to establish the need for anal mucosectomy and hand-sewn ileal pouch anastomosis.
Contrast-enhanced computed axial tomography (CAT) scan of the abdomen/pelvis assists the surgeon to decide on the feasibility of a single-incision laparoscopic approach. It also helps in identifying the exact location of large colonic or rectal neoplastic lesions, the potential involvement of adjacent organs or structures, and the potential presence of mesenteric adenopathy and/or metastases as well as inflammatory processes (phlegmon, abscess, fistula, or obstruction).
Endorectal ultrasound or rectal protocol magnetic resonance imaging (MRI) may assist with the staging of rectal carcinoma and identification of the anal sphincter muscle involvement. The latter would be a contraindication of a restorative proctocolectomy and may also delineate the anatomy of the anal sphincter in case of previous obstetric trauma or episiotomies.
Fecal incontinence—Wexner score preoperatively may assist with the diagnosis of fecal incontinence. Preoperative fecal incontinence may lead to poor functional outcome following an ileoanal pouch anastomosis.
Preoperative barium enema or small bowel follow-through contrast study may assist with the diagnosis of Crohn’s disease.
A carcinoembryonic antigen (CEA) level is obtained in malignancies as a tumor marker.
SURGICAL MANAGEMENT
Full bowel preparation is administered the day prior to surgery to reduce the weight and volume of the colon. This facilitates the laparoscopic handling of the colon and the extraction of the specimen via a small 3.5-cm single incision.
Obtain preoperative medical or pulmonary cardiac clearance as necessary.
Correct anemia, electrolyte imbalances, and malnutrition preoperatively as needed.
Wean off preoperative steroids to preferably less than 20 mg prednisone per day, if possible.
Give consideration to weight loss prior to surgery, especially in cases of chronic preoperative steroid usage. A short and thick ileal mesentery may preclude an ileoanal pouch anastomosis.
Intravenous (IV) antibiotics are administered prior to skin incision.
Instrumentation
A laparoscopic operating room (OR) table with steep tilting is used. Test maximum tilting prior to draping to assess patients’ secure positioning on the table (FIG 1).
Two laparoscopic high-definition screens, one on each side of the OR table, are used.
We use a bariatric length, 10-mm 30-degree camera. If needed, we use a right-angle adaptor for fiberoptic attachment to the camera to avoid conflict of the fiberoptic cord with other laparoscopic instruments. Using camera heaters and a smoke evacuator channel can avoid the need for repeated camera cleansing, leading to a decrease in operative length.

FIG 1 • Patient setup. The patient is secured to the table, with the arms tucked, a strap across the chest, and the legs on Yellofin stirrups. All pressure points are padded to avoid nerve and vascular injuries. The table tilt is tested prior to starting the case to ensure that the patient does not slide.
We use two bariatric length laparoscopic bowel graspers, laparoscopic scissors, and bariatric length laparoscopic 5- to 10-mm suction irrigation.
We prefer to use a bariatric length laparoscopic energy device such as the 43-cm LigaSure 5-mm device. Energy devices that produce excessive moisture or fog may impair visibility.
Laparoscopic Endoloop polydioxanone (PDS) for the ileocolic vascular pedicle
Staplers
Linear GIA 100-mm, triple blue staple lines for the ileal pouch formation
A 28- to 29-mm circular stapler for a stapled ileoanal pouch anastomosis
A 60-mm Endo GIA for distal division of the rectum as indicated
A second set of instruments is necessary for an extracorporeal anastomosis.
Patient Positioning
The patient is placed on modified lithotomy position on Allen stirrups with arms tucked (FIG 1). The patient is secured to the table, with foam pad placed under the patient’s torso and with Velcro or broad tape placed across the chest. Rolled surgical towel is placed under the sacrum to elevate the pelvis and assist with the coloanal or ileoanal anastomosis.
A Foley catheter is inserted and taped over the right thigh in order to avoid urethral trauma with the OR table tilting.
A bear hugger or other thermal device is applied to the chest and legs.
A protecting foam pad is placed over the head to protect from injury with laparoscopic instrument positioning.
We recommend using laparoscopic draping with side plastic bags or pockets to allow for bariatric instrument placement. All laparoscopic cords and energy device cords are brought out via the patient’s upper chest.
TECHNIQUES
DIAGNOSTIC LAPAROSCOPY—SINGLE MULTICHANNEL PORT TECHNIQUE
A 2.5-cm circular incision is performed at the right lower quadrant (RLQ) premarked temporary ileostomy site. Alternatively, a 3.5-cm periumbilical vertical midline incision is performed. A wound protector is inserted, followed by attachment of the single-incision laparoscopic surgery (SILS) port (FIG 2A,B).
Assemble all channels of the SILS port on the back table to avoid losing parts outside the sterile field. Insert the laparoscopic multichannel single port with a wound protector. Insufflate pneumoperitoneum carbon dioxide (CO2) to 15 mmHg of pressure.
Perform a diagnostic laparoscopy. The surgical assistant/camera holder and the surgeon stand by the patient’s right side when addressing the left colon, sigmoid, or rectum and by the patient’s left side when addressing the right colon. For the transverse colon mobilization, either side may be suitable or the surgeon may be positioned between the patient’s legs. Tilt the OR table to a steep Trendelenburg position and airplane it to the left or right for maximum exposure.
Minimize excursion/cluster effect around hands and camera between the surgical assistant and operating surgeon with adherence to the principle that the surgeon should position his or her assisting (nondominant hand) instrument’s distal tip (used for grasping, retracting, or suctioning) as close as possible to his or her operating (dominant hand) instrument’s (i.e., energy device) tip. This distance should be about 3 to 4 cm between the two instruments’ tips. For example, hold the ileocolic vascular pedicle just above the site of the division site rather than holing the cecum itself, which is far more distant from the pedicle. This technique allows achieving a wide angle between the two instruments outside the abdomen as they exit and cross via the single port, thus minimizing instrument conflict effect between the surgeon’s hands.
The assistant/camera holder will avoid conflict with the surgeon’s instruments outside the abdomen by holding the camera as far as possible from the surgeon’s hands and by using the camera’s 30-degree angulation for side view as well as the zoom-in option (FIG 2B).
Minimize the need for frequent laparoscopic instrument exchange, such as exchanging of graspers with monopolar laparoscopic scissors. Instead, consider using multiuse energy devices that provide dissection and sealing-cutting capabilities, thus allowing constant progress in the operating field and significant time saving.
The surgeon and the assistant can either switch sides during the various steps of the procedure or just rotate the single port clockwise or counterclockwise while the instruments stay in the abdomen under direct visualization with the camera, thus achieving different camera angles, better exposure, and better visualization.
The OR table can also be tilted accordingly during the various steps of the procedure to increase the exposure and prevent instrument conflict.
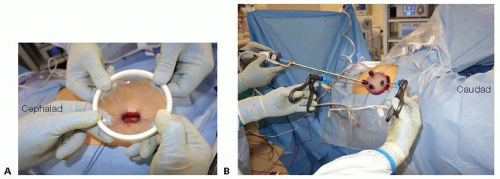 FIG 2 • SILS port placement and configuration. A. A wound protector is inserted in the RLQ at the diverting loop ileostomy site. B. A multiport channel with four working ports, insufflation port, and a smoke evacuator port is used. The port is assembled on a side table prior to insertion in the patient. The assistant/camera holder will avoid conflict with the surgeon’s instruments outside the abdomen by holding the camera as far as possible from the surgeon’s hands. |
MOBILIZATION OF THE RIGHT COLON: PRESERVATION OF THE ILEOCOLIC VASCULAR PEDICLE
The patient is positioned in a steep Trendelenburg position with the OR table tilted maximally toward the patient’s left side. The surgeon is standing on patient’s lower left side using a grasper in the nondominant hand and the energy device on the dominant hand. The camera holder stands cephalad to the surgeon.
If the omentum is adherent medially to the hepatic flexure or the ascending colon itself, we start the procedure with the dissection of the omentum off the colon. We may perform omentectomy by including the omentum with the transverse colectomy.
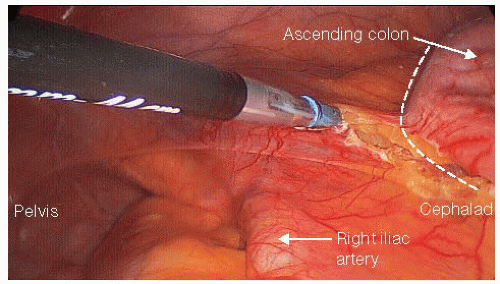
FIG 3 • Mobilization of the ileum and ascending colon. The mobilization starts by transecting the ileocecal retroperitoneal attachments (dotted line). The dissection will then proceed on a caudad to cephalad direction, eventually exposing the origin of the superior mesenteric artery and the third portion of the duodenum.
Dissect the terminal ileal retroperitoneal attachments and mobilize it toward the midline (FIG 3), exposing the origin of the superior mesenteric artery and the third and fourth portions of the duodenum. Morbidly obese patients require a generous terminal ileal medial mobilization to allow for a tension-free ileoanal pouch anastomosis.
Proceeding from a caudad to cephalad direction, dissect the ascending colon mesentery off its retroperitoneal attachments without entering Gerota’s fascia and preserving the right gonadal vessels and the right ureter intact. Dissect the ascending colon mesentery off the second and third portions of the duodenum in an atraumatic fashion.
Using an energy device, we hemostatically divide the ascending colon mesenteric vascular arcade while protecting the ileocolic vascular pedicle up to the mesenteric level of the ileocecal valve (FIG 4). This is critical to ensure a good blood supply to the pouch. Avoiding an ileocolic mesenteric bleeding or hematoma is crucial for preservation of the vascular supply to the ileal J-pouch.
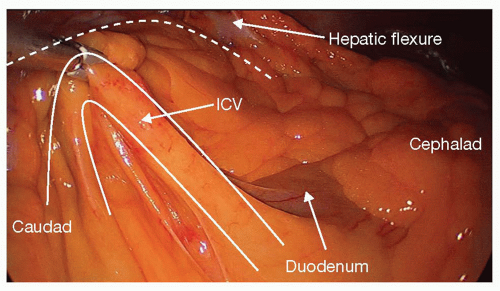
FIG 4 • Preservation of the ileocolic vessels (ICV). During the dissection of the right colon, it is critical to divide the mesentery close to the colonic wall (dotted line), preserving the ICV (here seen crossing over the third portion of the duodenum) intact. This will ensure excellent blood supply to the pouch.
Divide with the energy device the ascending colon mesentery flush to the ileocolic vascular pedicle (staying close to the colonic wall), up to the mesenteric border of the terminal ileum at the selected site of proximal intestinal division, just proximal to the ileocecal valve.
Proceed with laparoscopic division of the incidental right colonic artery/vein if present.
Mobilize the ascending colon medially by transecting the white line of Toldt.
MOBILIZATION OF THE TRANSVERSE COLON
The surgeon stands in between the patient’s leg. Place the patient on Trendelenburg and keep the OR table tilted to the left for the proximal transverse colon mobilization or to the right for the distal transverse colon and the splenic flexure mobilization. Alternatively, we may place the patient on reverse Trendelenburg for exposure and the assistant may use a laparoscopic grasper to assist with the retraction—“tenting”—of the transverse colon.
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


