Regenerative and Dysplastic Nodules
Sanjay Kakar, MD
Key Facts
Clinical Issues
RN: Regenerative nodule greater than 1 cm; most believed to be nonneoplastic
LGDN resemble RN morphologically but are clonal
HGDN: Preneoplastic lesion; likely precursor of HCC
Macroscopic Features
Greater than 1 cm but usually less than 3 cm
Microscopic Pathology
RN/LGDN: Plates 1-2 cells thick, portal tracts present, no architectural or cytologic atypia
HGDN: Plates focally up to 3 cells thick; small cell change with increased N:C ratio
Unpaired arterioles and pseudoacinar architecture can be present
Reticulin is preserved
May be focally lost in HGDN
Top Differential Diagnoses
Small cell change, high N:C ratio, pseudoacinar architecture, and unpaired arterioles favor HGDN over LGDN
Uniformly thick plates (> 3 cells) is most important feature distinguishing HCC from HGDN
Prominent pseudoacinar architecture, numerous unpaired arterioles and loss or fragmentation of reticulin favor HCC
Stromal invasion distinguishes early HCC from HGDN
Lack of CK7(+) ductular reaction is useful in demonstrating stromal invasion
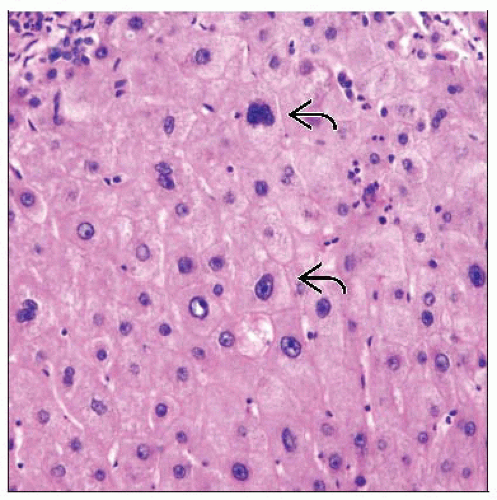 Large cell change is characterized by large hyperchromatic nuclei but preserved nuclear to cytoplasmic ratio  . This change is thought to be degenerative and not preneoplastic. . This change is thought to be degenerative and not preneoplastic. |
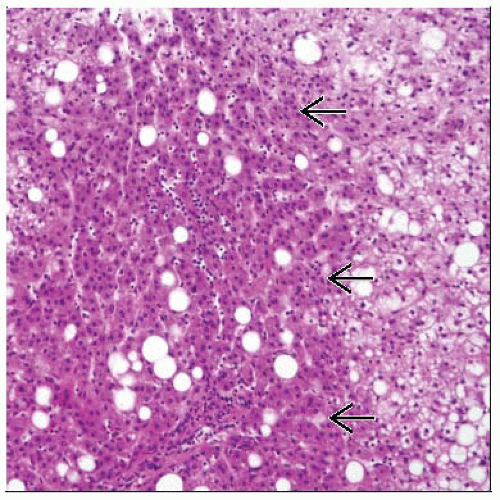 Small cell change (left 2/3 of image)  is characterized by small cells with high N:C ratio leading to increased cell density. When present in a nodule, it is the hallmark of HGDN. is characterized by small cells with high N:C ratio leading to increased cell density. When present in a nodule, it is the hallmark of HGDN. |
TERMINOLOGY
Abbreviations
Regenerative nodule (RN), macroregenerative nodule (MRN), low-grade dysplastic nodule (LGDN), high-grade dysplastic nodule (HGDN)
Synonyms
RN: Large regenerative nodule, macroregenerative nodule, adenomatous hyperplasia
HGDN: Borderline nodule, type II macroregenerative nodule, atypical adenomatous hyperplasia, atypical macroregenerative nodule
Definitions
Dysplasia: Abnormal histologic growth that does not fulfill criteria of malignancy
Dysplastic focus: Cluster of dysplastic hepatocytes less than 1 cm in diameter
Dysplastic nodule: Cluster of dysplastic hepatocytes greater than 1 cm in diameter
Regenerative nodule: Large (greater than 1 cm) nodule usually seen in context of cirrhosis
No reliable gross or histologic criteria for distinguishing RN from LGDN, thus they will be considered together here
LGDN thought to represent clonal proliferation of hepatocytes although likelihood of progression to carcinoma is unclear
Most RN are probably not preneoplastic
HGDN: Nodule with atypical cytologic and architectural features believed to be precursor of carcinoma
Large cell change (formerly large cell dysplasia)
Large hepatocytes with nuclear enlargement, hyperchromasia, prominent nucleoli, often multinucleated
Abundant cytoplasm and hence normal nuclear cytoplasmic ratio
Very common in cirrhotic liver
Formerly thought to be precursor of hepatocellular carcinoma (HCC)
No longer considered preneoplastic but rather regenerative or degenerative phenomenon
Low proliferation rate and absence of P53 mutations also do not support preneoplastic process
Small cell change (formerly small cell dysplasia)
Small hepatocytes with increased nuclear to cytoplasmic ratio and hyperchromatic nuclei
High proliferative activity and P53 overexpression can occur
Likely to be preneoplastic when occurring in expansile nodules
Poorly defined or diffuse areas of small cell change without nodular configuration may represent regenerative phenomenon
Small cell regenerative foci common in biliary disease, unlikely to be preneoplastic
CLINICAL ISSUES
Presentation
Occur in setting of cirrhosis, usually in background of hepatitis B, hepatitis C, alcoholic liver disease, hemochromatosis
Uncommon in chronic biliary diseases
Can occasionally occur in chronic liver disease without fully developed cirrhosis
Can occur in noncirrhotic liver in Budd-Chiari syndrome, portal vein thrombosis, or regeneration after necrosis
May be detected at autopsy, transplantation, or by imaging
Serum AFP is normal or mildly elevated
Treatment
Prognosis
RN: Most RN regress or remain unchanged on imaging follow-up and thus are probably not preneoplastic
LGDN: Unclear but probable low likelihood of progression as well
Difficult to ascertain prognosis since it is difficult to clearly define entity LGDN
HGDN
Preneoplastic lesion, likely precursor of HCC
Allelic imbalance is seen in > 80% compared to 15% of regenerative nodules
Most remain stable or regress on follow-up; progression to HCC in 10-15%, but this data is based on limited studies
MACROSCOPIC FEATURES
Regenerative Nodules (Including LGDN)
Larger than typical cirrhotic nodules
By definition > 1 cm but usually < 3 cm
May be pale yellow to tan compared to other cirrhotic nodules; some can be bile-stained
Sharply circumscribed and bulge on cut section
High-Grade Dysplastic Nodule
Similar gross appearance as RN/LGDN
Some HGDN are not well circumscribed and may show irregular border
MICROSCOPIC PATHOLOGY
Histologic Features
Regenerative nodule
Resemble cirrhotic nodules; cell plates are 1-2 cells thick
Reticulin framework is intact
Portal tracts are usually present within nodule, and ductular reaction may be prominent
Occasional unpaired arterioles may be seen, but this is not prominent finding
Hepatocytes typically appear normal; mild variation in cell size and scattered large cell change can be present
Specific morphologic features for low-grade dysplasia have not been established
May be indistinguishable from lesions formerly called MRN in the absence of clonality studies
May contain Mallory-Denk bodies, bile, clear cell changes, iron, copper, and fat
CD34 shows patchy sinusoidal staining at edge; occasional nodules can show more diffuse expression
Nodules are negative for α-fetoprotein and GPC with rare exceptions
No histologic criteria to distinguish RN from LGDN
High-grade dysplastic nodule
HG dysplastic changes may involve entire nodule or present as one or more dysplastic foci within nodule
By definition, atypical features do not fulfill criteria of diagnosis of HCC
Focal areas with up to 3-cell thick plates may be present (normal cell plates are typically 1-2 cells thick)
Reticulin network is normal or focally decreased
Pseudoacinar architecture can be present but is usually not diffuse
Portal tracts are present within nodule
Scattered unpaired arterioles are present but not as numerous as in HCC
Small cell change with increased nuclear to cytoplasmic ratio is a characteristic feature
Results in nuclear crowding and increased nuclear density
Large cell change can be seen but is neither sufficient nor necessary for diagnosis
May contain Mallory-Denk bodies, fat, clear cell change, cytoplasmic basophilia, bile
Tend to lack iron (in contrast to MRN, where iron deposits are more common)
CD34 shows patchy sinusoidal staining, usually at edge; occasional nodules can show more diffuse expression
α-fetoprotein is negative
Glypican-3 (GPC) expression is variable; diffuse strong expression strongly favors HCC
DIFFERENTIAL DIAGNOSIS
Other Regenerative Nodules
By definition, size > 1 cm differentiates RN from other cirrhotic nodules
Hepatic Adenoma
Rarely, RN may lack portal zones and resemble hepatic adenoma
True adenomas rarely, if ever, occur in cirrhotic liver
RN/LGDN vs. HGDN
Cytologic abnormalities like small cell change and nuclear atypia favor HGDN
Architectural abnormalities like pseudoacinar architecture, focal reticulin loss, and unpaired arterioles favor HGDN
HGDN vs. Well-Differentiated HCC
Cell plates more than 3 cells thick are most important feature distinguishing HCC from HGDN
Prominent pseudoacinar architecture and numerous unpaired arterioles are typical of HCC
Loss or fragmentation of reticulin network strongly favors HCC
CD34 is typically diffuse in HCC and patchy in HGDN, but considerable overlap exists
CK7(+) ductular reaction present around over 50% of circumference of HGDN in most cases; this is focal or lost in most HCC
GPC expression favors HCC, especially if strong and diffuse
GPC expression described in 7-22% of HGDN also
HGDN vs. Early HCC (Early Well-Differentiated HCC or Vaguely Nodular HCC)
Characteristic feature of early HCC is stromal invasion leading to vaguely nodular appearance
Stromal invasion can occur at nodule-parenchymal or nodule-septal interface within nodule or at periphery
Since stromal invasion can be focal, distinction from HGDN on biopsy may not be possible
Lack of CK7(+) ductular reaction can be useful in demonstrating stromal invasion
Uniformly thick plates (> 3 cells), prominent pseudoglands, and loss of reticulin are typical of progressed HCC; may not be seen in early HCC
Immunohistochemistry
GPC expression is more often seen in early HCC than HGDN
Glutamine synthetase (GS), a downstream gene in β-catenin pathway, is diffusely positive in many early HCC (up to 70%)
10-15% of HGDN can be positive (usually focal)
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


