Pyloric Exclusion and Duodenal Diverticulization
Injuries of the duodenum can be difficult to manage. In this chapter, exposure of the duodenum from the pylorus to the suspensory ligament of duodenum (ligament of Treitz) and two useful maneuvers for managing complex injuries to the duodenum are covered.
Duodenal injuries are rarely isolated. Careful assessment of the adjacent pancreas, bile duct, colon, and neighboring vascular structures is an essential component of management.
List of Structures
Stomach
Pylorus
Duodenum
First portion (duodenal ampulla or bulb)
Second portion
Third portion
Fourth portion
Pancreas
Head of pancreas
Suspensory ligament of duodenum (ligament of Treitz)
Gallbladder
Bile duct
Colon
Ascending (right) colon
Hepatic flexure
Cecum
Transverse colon
Embryologic Terms
Foregut
Midgut
Hindgut
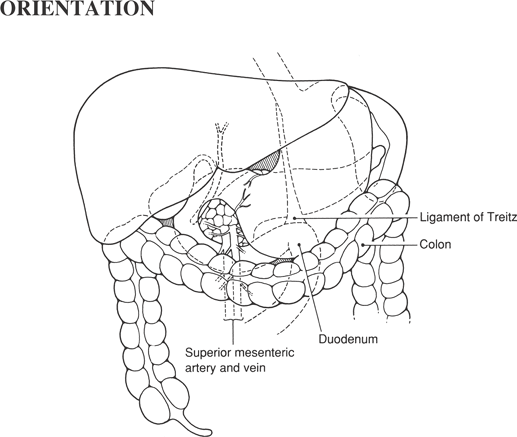
Exposure of the Duodenum (Fig. 57.1)
Technical Points
First, mobilize the hepatic flexure of the colon by incising the lateral peritoneal attachments at the hepatic flexure. Make a small window in the peritoneum with Metzenbaum scissors, then pass the fingers of the nondominant hand behind the colon, sweeping the peritoneum up and thinning it out. Divide it with electrocautery. Often, there are filmy adhesions extending to the gallbladder; divide these by sharp dissection.
If you anticipate the need to expose the entire duodenum, pass your nondominant hand down behind the ascending (right) colon and divide the lateral peritoneal reflection all the way down past the cecum. Lift the ascending (right) colon with its mesentery, sharply dividing any filmy adhesions between the colon and retroperitoneum. The third portion of the duodenum will be visible as the colon is swept medially. Elevate the ascending (right) colon and the mesentery of the small intestine (carefully preserving the superior mesenteric vessels) and swing them toward the left shoulder of the patient. The anterior surface of the duodenum from the pylorus to the suspensory ligament of duodenum (ligament of Treitz) should now be visible.
Mobilize the duodenum and head of the pancreas using a wide Kocher maneuver to gain access to the lateral and posterior surfaces of the duodenum in these regions. The fourth portion of the duodenum may be similarly mobilized by incising the antimesenteric border.
Anatomic Points
This procedure is made necessary, as well as technically possible, by the embryologic rotation of the gut. A knowledge of this developmental process enables a rational approach to the procedure.
The gut can be divided into foregut, midgut, and hindgut. For the purposes of the general surgeon operating on the abdomen, these divisions can be defined as follows: the foregut is that portion of the gut supplied by the celiac artery, the midgut is that portion supplied by the superior mesenteric artery, and the hindgut is that portion supplied by the inferior mesenteric artery. Foregut derivatives in the abdomen include the distal esophagus, the stomach, and the duodenum to just distal to the major duodenal papilla. The liver and biliary apparatus arise as the hepatic diverticulum from the terminal foregut, whereas the pancreas arises from a diverticulum of the hepatic diverticulum and from a separate dorsal pancreatic bud. Midgut derivatives include the rest of the duodenum, all of the small intestine, the appendix, the cecum, the ascending colon, and the proximal two-thirds of the transverse colon. Hindgut derivatives include the distal one third of the transverse colon, the descending colon, the sigmoid colon, the rectum, and the anal canal to the anal valves.
 |
The development of the abdominal gastrointestinal tract can be understood as a consequence of two phenomena. One of these is differential growth of the gut components in comparison to each other and to the developing peritoneal cavity. The other is the fusion and later degeneration, of apposed serosal surfaces. What follows is a conceptual description of some of the surgically relevant facets of the development of the infradiaphragmatic gastrointestinal system.
Initially, the gut is a midline intraperitoneal tube suspended from the dorsal body wall along its entire length by the dorsal mesentery. A ventral mesentery attaches the foregut to the anterior body wall from the umbilicus to the diaphragm, carrying the left umbilical vein from the umbilicus to its ultimate union with the caval system. As the fusiform dilatation destined to become stomach begins to develop by rapid elongation, the duodenum assumes the form of a C-shaped loop, with its convexity directed ventrally. Soon after these structures begin to be recognizable, the stomach changes its position by rotating 90 degrees to the right about its longitudinal axis. The end result of this rotation is that the right side of the stomach becomes the definitive posterior side and the left side becomes the definitive anterior side. Moreover, the original dorsal border becomes the greater curvature and the ventral border becomes the lesser curvature. As a result of the positional changes of the stomach, the C-loop of the duodenum rotates about a longitudinal axis so that the convex border becomes its definitive right border. This causes the right side of the duodenum and the right leaf of the mesoduodenum to be in apposition to the dorsal parietal peritoneum. The apposed serosal surfaces soon fuse and then degenerate, placing the bulk of the duodenum and pancreas, which develops primarily within the mesoduodenum, in a retroperitoneal position.
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


