The spectrum of pulmonary neuroendocrine tumors encompasses several types of neoplasms, some encountered more frequently than the others. Their classification is quite complex, as is the terminology (see Chapter 1, Taxonomy). Not all neuroendocrine tumors are identified in cytologic specimens, especially the preneoplastic neuroendocrine lesions that are included in the most recent World Health Organization/International Association for the Study of Lung Cancer (WHO/IASLC) (2004) classification of the lung tumors.
CLASSIFICATION OF PULMONARY NEUROENDOCRINE TUMORS
The classification of pulmonary neuroendocrine tumors as a whole has generated considerable debate over the years. A recent publication (Moran et al., 2009) consolidated several recommended classifications and proposed a three-tier one that is considered practical.
For typical carcinoid tumor, the recommended terminology would be grade I neuroendocrine carcinoma (NEC) or well-differentiated NEC or low-grade NEC with fewer than 3 mitotic figures per 10 high-power field (HPF) and only punctate necrosis.
For atypical carcinoid tumor, the recommended terminology would be grade II NEC or moderately differentiated NEC or intermediate grade NEC with more than 3 mitotic figures per 10 HPF and necrosis, usually comedo-like necrosis.
Grade III NEC or poorly differentiated NEC or high-grade NEC to include
Small cell carcinoma (tumor with or without posi tive neuroendocrine markers and with more than 10 mitotic figures per 10 HPF and necrosis)
Large cell neuroendocrine carcinoma (LCNEC): tumor with positive neuroendocrine markers and tumor with morphologic features of neuroendocrine and negative staining for neuroendocrine markers.
The traditional four-tier classification of pulmonary neuroendocrine neoplasms included (1) typical carcinoid tumor, (2) atypical carcinoid tumor, (3) LCNEC, and (4) small (Appendix) cell carcinoma. This classification is retained by WHO (2004) and is followed in this chapter. The corresponding new terminology is given in parenthesis.
The pulmonary NECs comprise up to 20% of all pulmonary malignancies. They present a spectrum of morphologic features ranging from benign-appearing, uniform cellular patterns to highly anaplastic ones. Their biologic behavior likewise ranges from that of a protracted course in typical carcinoid tumors to an aggressive one with a fatal outcome as seen in large cell neuroendocrine and small cell carcinomas. Despite the differences in their biologic behavior, pulmonary neuroendocrine tumors share several properties, such as morphologic features, growth patterns, presence of cytoplasmic secretory granules, expression of broad-spectrum neuroendocrine markers, and expression of specific peptide hormones and amines. See Table 3.10 for the summary of their clinicopathologic and cytopathologic features.
PULMONARY CARCINOID TUMORS (NEC, GRADE I, WELL-DIFFERENTIATED NEC, LOW-GRADE NEC)
Typical carcinoid tumors are neoplasms with low malignant potential, accounting for 1% to 2% of all primary lung cancers. The carcinoid tumors are derived from neuroendocrine cells (Kulchitsky cells) known to exist in normal airways. Pulmonary carcinoid tumors occur more frequently in women, at any age, with a mean of 55 years. There is no association with smoking.
The majority of patients harboring carcinoid tumors are asymptomatic. Those with centrally located tumors may present with hemoptysis, dyspnea, and postob-structive pneumonia. Roughly 2% to 7% of patients with carcinoid tumors develop carcinoid syndrome resulting from increased production of serotonin. The majority of the patients with carcinoid syndrome have hepatic metastasis. Some patients with carcinoid tumors develop Cushing syndrome due to ectopic production of ACTH. Hilar lymph nodes are involved in roughly 20% of the cases and 5-year disease-free survival is reported to be 100%. In general, carcinoid tumors follow an indolent course. However, they do metastasize to the distant sites, such as liver, bones, serous cavities, and skin.
GROSS AND HISTOLOGIC FEATURES
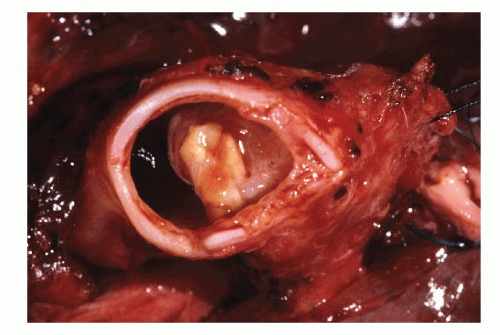
Carcinoid tumors are equally located centrally, in the mid portion of the lung, and peripherally. Central carcinoid tumors frequently present as a large endobronchial exophytic fleshy polypoid mass with a smooth surface protruding into the bronchial lumen (Fig. 3.1). The tumor infiltrates the underlying tissues beyond the cartilage plates into the surrounding parenchyma. The cut surface may appear tan-yellow to red. Gross necrosis and hemorrhage are not the features of a typical carcinoid tumor. Peripheral carcinoid tumors are situated in the subpleural parenchyma and anatomically are not related to a bronchus or a bronchiole. They are circumscribed, nonencap-sulated, may be multiple, and tend to be smaller in size than the central carcinoids.
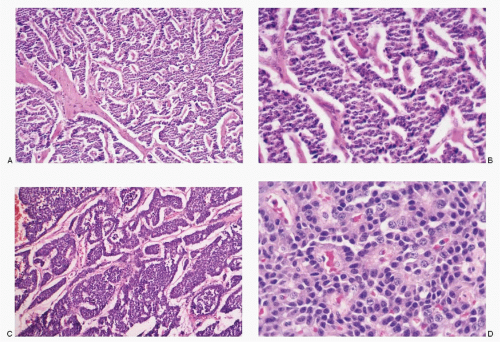
Histologically, the typical carcinoid tumor consists of uniform small, round to cuboidal cells with varied growth patterns that are characteristic of neuroendocrine tumors (neuroendocrine growth pattern) (Fig. 3.2). The neoplastic cells are compactly arranged in well-defined alveoli, nests, islands, trabeculae, and ribbons separated by delicate vascular stroma. Other morphologic patterns include pseudoglandular, rosettes, and sometimes palisading arrangement at the periphery of the islands of tumor cells. Papillary pattern may rarely be encountered. The nuclei of the carcinoid tumor cells are round to oval with coarsely granular, stippled, salt-pepper chromatin with inconspicuous nucleoli. The cell borders are well-defined. The cytoplasm is variable, scant to moderate, pale to eosinophilic, and at times clear. Several morphologic variants have been described, namely, oncocytic, clear cell, spindle cell, and melanotic.
Spindle cell carcinoid tumors are unusual occurrences, comprising 5% of all pulmonary carcinoid tumors. They tend to be peripheral and are not anatomically related to the airways. Spindle cell carcinoids are well circumscribed and nonencapsulated. Tumor nodules may infiltrate into the surrounding parenchyma. Microscopically, spindle cell carcinoids are composed of swirling bundles of short to long spindle cells with round to oblong nuclei containing salt-pepper type chromatin, a characteristic feature of neuroendocrine tumors (see Fig. 3.15). Nucleoli are inconspicuous. The cells of spindle cell carcinoids have indistinct cell borders and possess a modest amount of pale eosinophilic cytoplasm. Spindle cell carcinoid tumors may contain areas with morphology of a typical carcinoid tumor.
CYTOPATHOLOGIC FEATURES
The cytologic specimens for the diagnosis of carcinoid tumors include those obtained via bronchoscopy such as bronchial brushings, washings, bronchoalveolar lavage, and transbronchial fine needle aspiration (FNA) biopsies of the lung or mediastinal lymph nodes. Transthoracic fine needle biopsy procedure under computed tomography (CT) guidance is sometimes utilized. Fine needle biopsies are also utilized for metastatic lesions from the carcinoid tumors beyond the thoracic cavity. Spread to the serous membranes may be diagnosed by examination of the serous effusion fluids.
Carcinoid tumors rarely, if ever, shed cells spontaneously in airways since they are mostly in submucosal location. Sputum samples therefore are usually nondiagnostic. Bronchial brushings, washings, bronchoalveolar lavage, and aspiration biopsies are useful in establishing the diagnosis. Bronchial carcinoid tumors in subepithelial locations cannot be sampled by brushing if the overlying mucosa is intact. Bronchial brushings in such instances are often nondiagnostic.
The cells of typical carcinoid tumors present a distinctive pattern (Table 3.1; Figs. 3.3,3.4,3.5,3.6,3.7,3.8,3.9,3.10,3.11,3.12,3.13 and 3.14). They occur as loosely cohesive cells in a dispersed fashion or form syncytial tissue fragments with various architectural patterns such as nests, trabeculae, and occasionally a pseudoacinar or a pseudopapillary pattern. Strikingly uniform, small, round to cuboidal, sometimes plasma-cytoid cells with typical salt-pepper chromatin granules are a hallmark of carcinoid tumors (Fig. 3.3B,C). The nuclear membranes are smooth and regular. Nucleoli are inconspicuous, and nuclear molding, stretch artifacts, karyorrhexis, or mitotic figures are not present. The cells of typical carcinoid tumors in cytologic preparations generally exhibit poorly defined cell borders and insignificant or scant pale cytoplasm in contrast to histologic sections. Occasionally, the cells may exhibit pale somewhat bubbly cytoplasm resembling well-differentiated adenocarcinoma cells (Fig. 3.8A,B) and are distinguished by positive reactivity to neuroendocrine markers (Fig. 3.8C). Abundant granular cytoplasm in the oncocytic variant of a carcinoid tumor has been misinterpreted as a granular cell tumor. On rare occasions, carcinoid tumor cells may demonstrate a very pleomorphic cell pattern with an admixture of plasmacytoid and short spindle cells with cytoplasmic processes, reminiscent of medullary thyroid carcinoma or a paraganglioma (Fig. 3.7A,B). The background is clean, and necrosis is absent. A perithelial pattern with carcinoid cells attached to the capillaries is quite characteristic in fine needle aspirates (Fig. 3.9C).
Fig. 3.1: Gross photograph of an endobronchial tumor, partially obstructing the lumen, histologically confirmed as a typical carcinoid tumor.
Spectrum of Histologic Features of Typical Carcinoid Tumors
Fig. 3.2: A: A medium-power view of a carcinoid tumor exhibiting a trabecular pattern, formed by uniform cuboidal cells. Note that the tumor is richly vascular, with trabeculae separated by sinusoids (H&E). B: Another example showing broad islands of uniform cells, separated by delicate stroma. There is a pseudoglandular pattern (H&E). C: Uniform cuboidal cells, arranged around the capillaries with a pseudoacinar pattern (H&E). D: Branching trabeculae formed by uniform cells with nuclei containing granular chromatin (H&E).
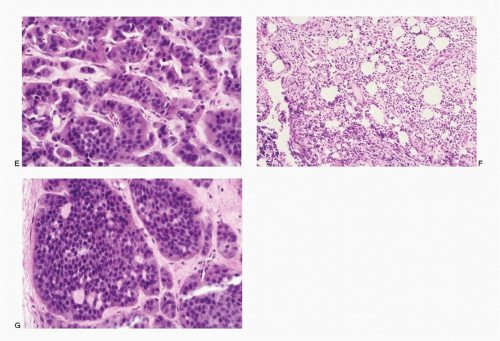
Fig. 3.2:(continued)E: Higher magnification showing nests of carcinoid tumor cells (H&E). F: Histologic section of a typical carcinoid tumor with very small loosely cohesive cells with a diffuse pattern (H&E). G: Histologic section of a carcinoid tumor showing large islands of neoplastic cells with a glandular pattern (H&E).
TABLE 3.1. CYTOPATHOLOGIC FEATURES OF CARCINOID TUMORS
Cellularity
Variable, generally very cellular
Presentation
Cells dispersed, isolated, in loosely cohesive groups or in syncytial tissue fragments as cords, nests, or anastomosing ribbons with occasional acinar pattern; dispersed pattern more frequent in brushings and washings; perivascular location with cells lining capillaries in FNA specimens
Cells
Small, round to cuboidal; cell borders well to poorly defined; uniform, monotonous pattern with occasional large pleomorphic forms; short to long spindle cells in some peripheral carcinoids
Nucleus
Round to oval in typical carcinoids; oblong in spindle cell carcinoids; smooth nuclear borders; N/C ratios generally high; chromatin coarsely granular, salt-pepper type; nucleolus +/-; no nuclear molding; no karyorrhexis; mitoses absent; no stretch artifacts
Cytoplasm
Scant to moderate; pale occasionally foamy (mistaken for adenocarcinoma), rarely oncocytic
Background
Clean
Histochemistry
Argyrophilic
Immunoprofile
Reactive to neuroendocrine markers and (CAM5, 2 and CK7), TTF-1, CD56
Ultrastructure
Membrane bound neurosecretory granules
Modified from Kini SR. Color Atlas of Pulmonary Cytopathology. New York: Springer-Verlag Inc.; 2002.
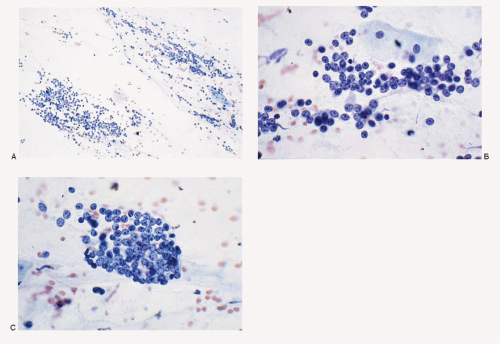
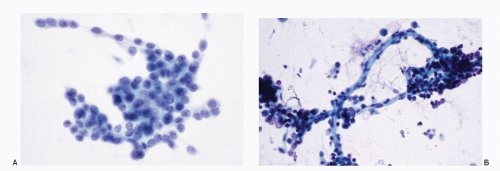
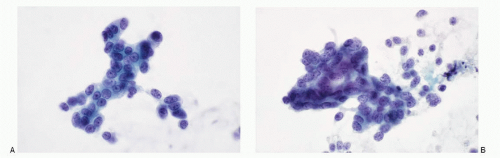
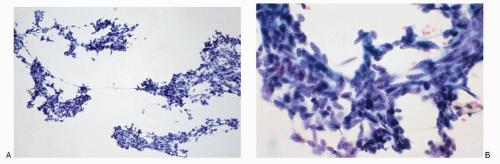
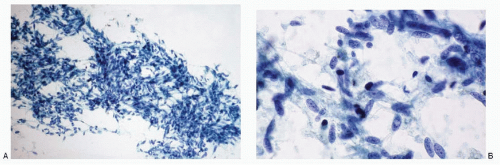
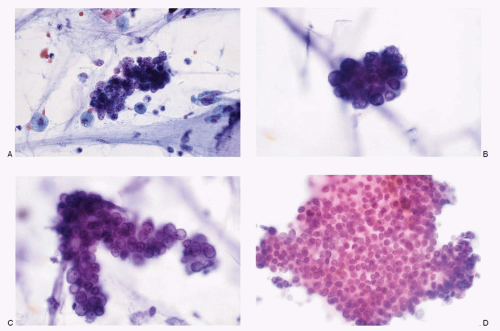
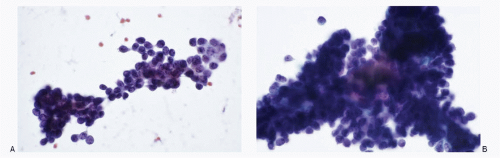
Fig. 3.3: Bronchial Brushings, Direct Smear. A: Low-power view, showing a cellular smear, with streaks of small uniform cells. B: Higher magnification showing well-preserved cells with a strikingly uniform size. These cells are round, with poorly defined cell borders and indiscernible cytoplasm. The nuclei have granular (salt-pepper) chromatin and nucleoli are conspicuous. Note that there is no nuclear molding. C: Different field from the same case with cells presenting similar cytomorphology. Note the typical salt-pepper chromatin.
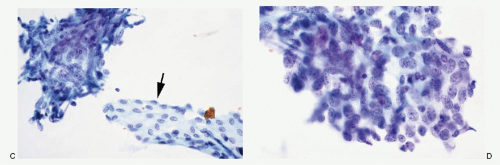
Fig. 3.4: Typical Carcinoid Tumor. A: Direct smear of bronchial brushings showing a characteristic pattern of typical carcinoid tumor with uniform, small cuboidal to round cells. Their nuclei are likewise uniform with granular chromatin and inconspicuous nucleoli. The cytoplasm is indistinct. B: Another example of a typical carcinoid tumor identified in bronchial brushings. The neoplastic cells are small round, resembling lymphoid cells with high N/C ratios. Note the densely stained chromatin. Note the perivascular location of the neoplastic cells.
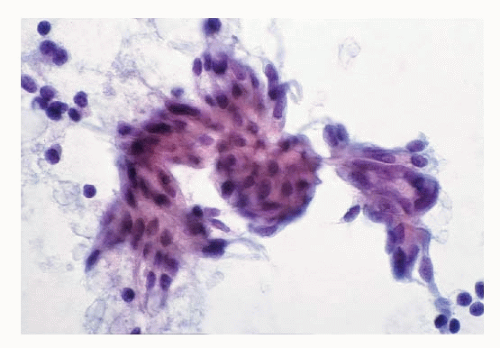
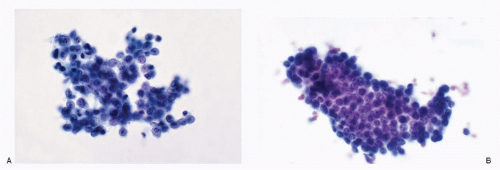
Fig. 3.5: Typical Carcinoid Tumor. A, B: Direct smears of the bronchial brushings. The neoplastic cells are small to medium-sized forming broad trabeculae. Their nuclei exhibit salt-pepper chromatin, very typical of neuroendocrine neoplasms.
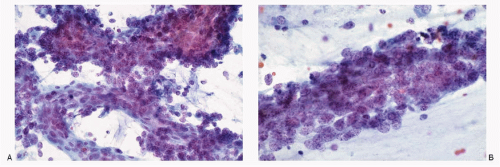
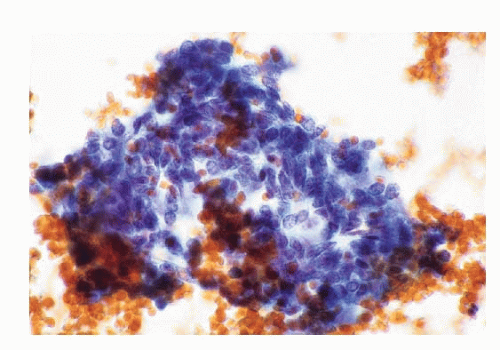
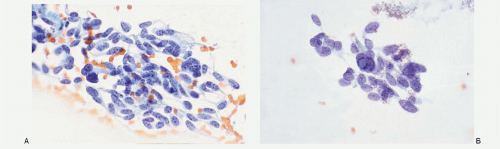
Fig. 3.6: Typical Carcinoid Tumor. Direct smears of the bronchial brushings. A, B: The smears demonstrate tissue fragments of medium-sized malignant cells with nuclei containing fine granular chromatin and prominent nucleoli. These cells possess appreciable pale to foamy cytoplasm, suggesting adenocarcinoma. C: Staining for chromogranin is strongly positive, confirming the neuroendocrine nature.
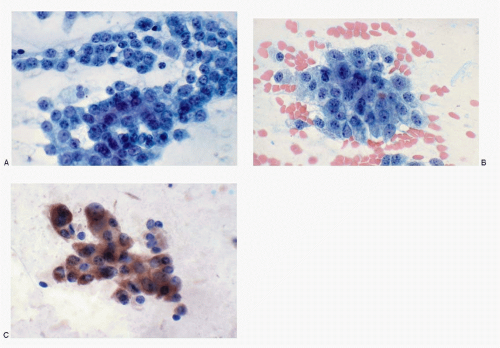
Fig. 3.7: Typical Carcinoid Tumor. Direct smears of the bronchial brushings. A, B: The smears demonstrate loosely cohesive, very pleomorphic neoplastic cells ranging from medium to large, round to polygonal containing abundant dense cytoplasm. Their nuclei are eccentric with coarse chromatin. Some cells are binucleated. Note the cytomorphology strongly resembles that of a medullary thyroid carcinoma. No history of thyroid carcinoma was available. C: Strong positive reactivity to chromogranin. Bronchial biopsy and the excision confirmed a carcinoid tumor.
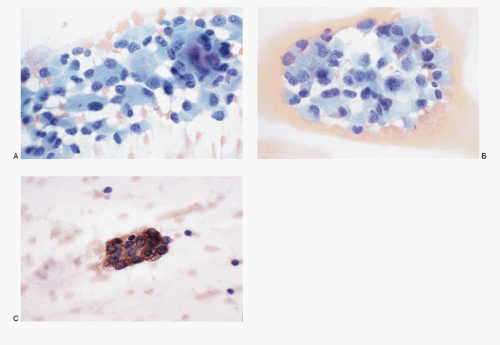
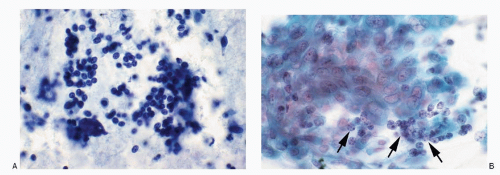
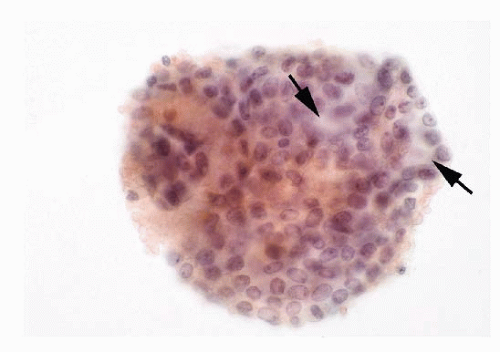
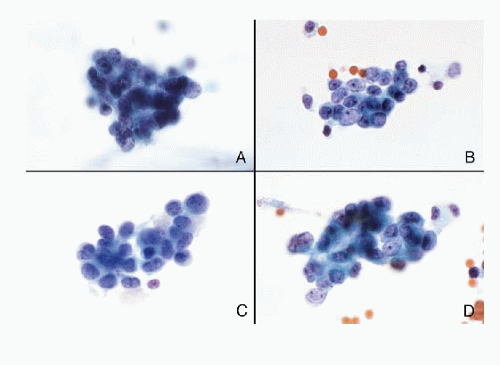
Fig. 3.8: Typical Carcinoid Tumor. Bronchial washings. A: This smear shows a large number of deeply stained cells with poorly defined cell borders, indistinct cytoplasm with high N/C ratios. These cells resemble lymphoid cells. There is no nuclear molding. A diagnosis of carcinoid tumor, however, was made earlier on the smears of the direct brushings. B: Different field from the same preparations. The carcinoid tumor cells are small, few in numbers but well-preserved, dispersed, obscured by bronchial epithelial cells, and can be easily overlooked (arrows). Note the classic morphology seen in direct smears is not seen in washings or lavage.
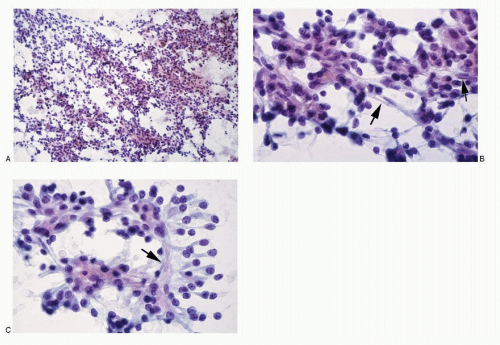
Fig. 3.9: Typical Carcinoid Tumor. FNA of a lung mass. A: Medium-power view of a very cellular aspirate consisting of loosely cohesive small cells. B: Higher magnification shows neoplastic cells that are isolated in loosely cohesive groups and syncytial tissue fragments. The cells are medium-sized with well to poorly defined cell borders and scant to moderate cytoplasm. The nuclear chromatin is granular to dense. Note the capillary traversing as seen by the elongated endothelial cell (arrows). C: This field shows carcinoid tumor cells attached to the blood vessels (arrow).
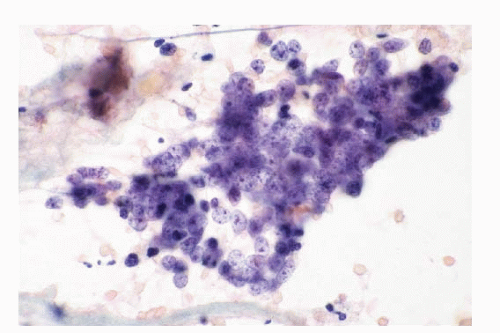
Fig. 3.10: Typical Carcinoid Tumor. FNA of a lung mass showing a syncytial tissue fragment of uniform cuboidal to round cells with scant cytoplasm and typical nuclear pattern with salt-pepper chromatin.
Fig. 3.11: Typical Carcinoid Tumor. FNA of a lung mass. This syncytial tissue fragment of neoplastic cells consists of cells with varied nuclear morphology. Some nuclei contain fine granular chromatin with occasional nucleoli suggest a possibility of an adenocarcinoma.
Fig. 3.12: Typical Carcinoid Tumor. FNA of a lung mass. A, B: The aspirate is very cellular consisting of medium-sized round cells with high N/C ratios. The nuclear chromatin is granular and the cytoplasm is scant. The excised tumor confirmed the diagnosis of a typical carcinoid tumor.
Fig. 3.13: Typical Carcinoid Tumor. FNA of lung nodule showing a syncytial tissue fragment of carcinoid tumor cells. The neoplastic cells are small to medium-sized, with poorly defined cell borders. The nuclei are uniform with granular chromatin. No nucleoli are present. Note the pseudoacinar pattern (arrows), which may be misinterpreted as an adenocarcinoma (see Fig. 3.24D).
Fig. 3.14: Typical Carcinoid Tumor. A, B: FNA of a lung mass. These well-defined syncytial tissue fragments of neoplastic cells that are cuboidal with uniform nuclei containing granular chromatin strongly suggest a carcinoid tumor, but must be differentiated from an adenocarcinoma.
The cytologic diagnosis of spindle cell carcinoid is offered from specimens obtained via fine needle biopsies, as these tumors are usually peripheral and may not be accessible to brushings. As seen in histologic sections (Fig. 3.15), cytologically, spindle cell carcinoid tumors demonstrate short to long spindle cells, discrete, in groups, or in fascicles with cytoplasmic processes (Figs. 3.16,3.17 and 3.18). Their nuclei are round to oblong with smooth nuclear membranes containing typical salt-pepper type chromatin and inconspicuous nucleoli. The cytoplasm is pale and variable. Spindle cell carcinoid tumors may be associated with cells presenting the cytomorphology of a typical carcinoid (Fig. 3.17D). In aspiration biopsy specimens, the spindle cell carcinoid tumors must be differentiated from neoplasms that are composed of spindle cells, for example, soft tissue tumors, squamous carcinoma with spindle cell pattern, metastatic medullary thyroid carcinoma, malignant melanoma with a spindle cell pattern, and malignant mesothelioma with sarcomatous pattern (Table 3.2; Figs. 3.19 and 3.20).
HISTOCHEMISTRY
The cells of pulmonary carcinoid tumors are argyrophilic.
IMMUNOPROFILE
The carcinoid tumor cells are reactive to neuroendocrine markers, cytokeratin and TTF-1, and CD56.
ULTRASTRUCTURE
Ultrastructurally, the carcinoid tumor cells demonstrate dense core neurosecretory granules.
DIAGNOSTIC ACCURACY OF PULMONARY CARCINOID TUMORS
Adequacy of the specimen and optimal cytopreparation are essential for an accurate cytologic diagnosis (Figs. 3.21,3.22 and 3.23). Scant specimen with dispersed cells may result in a false-negative diagnosis (Figs. 3.22 and 3.23). The carcinoid tumors are often submucosal in location and do not yield to brushings. In bronchial washings, the carcinoid tumor cells tend to shrink and are not easily recognized (Fig. 3.8). The bronchial epithelium overlying a submucosal lesion may undergo squamous metaplasia. With varying degrees of cellular and nuclear atypia, the brushings of this metaplastic squamous epithelium may be interpreted as squamous carcinoma, resulting in a false-positive diagnosis (Fig. 3.21A-C).
DIFFERENTIAL DIAGNOSES OF PULMONARY CARCINOID TUMORS
The differential diagnostic possibilities of pulmonary carcinoid tumors include all the lesions both nonneoplastic and neoplastic that are composed of small cells as well as other neuroendocrine tumors (Table 3.3).
The benign entities, such as reserve cell hyperplasia, bronchial epithelial cell (columnar cell) hyperplasia, lymphocytes, and alveolar lining cells (in washings and lavage specimens), may mimic the cells of carcinoid tumor (see Figs. 3.61 and 3.63,3.64 and 3.65). Among the malignant neoplasms with a small cell pattern, the diagnostic considerations are other neuroendocrine tumors, namely atypical carcinoid, small cell carcinoma, LCNEC, malignant lymphoma, adenoid cystic carcinoma, poorly differentiated squamous carcinoma and its basaloid variant, primary and metastatic adenocarcinomas, and malignant melanoma (see Figs. 3.60,3.61,3.62,3.63,3.64,3.65,3.66,3.67,3.68,3.69 and 3.70). Pulmonary adenocarcinomas with a small cell pattern may be extremely difficult to differentiate from cells of carcinoid tumors (Fig. 3.24).
In addition to the above diagnostic entities, neuroendocrine tumors involving the mediastinal structures such as thymus, lymph nodes, or soft tissues must be considered in specimens obtained by transbronchial fine needle biopsy. These include thymic carcinoids, thymomas and thymic carcinomas, metastatic malignant melanoma, and in younger patients, primitive neuroectodermal tumors (PNETs).
Fig. 3.15: A, B: Histologic sections of a spindle cell carcinoid tumor, showing a solid growth pattern with closely packed spindle cells. Note the typical salt-pepper chromatin (H&E).
Fig. 3.16: FNA of a Peripheral Lung Mass Diagnosed as a Spindle Cell Type Carcinoid Tumor. Note the closely packed oblong to short spindle cells with deeply staining granular chromatin. The N/C ratios are high and the cytoplasm is insignificant.
Fig. 3.17: FNA of a Lung Mass. A: Low-power view of a very cellular aspirate showing several tissue fragments. Spindle cell pattern can be appreciated even at this power. B: Higher magnification showing delicate spindle cells with elongated slender nuclei containing typical salt-pepper chromatin.
Fig. 3.17:(continued)C: This field depicts spindle cells containing salt-pepper chromatin and a very uniform pattern. Note a tissue fragment of benign mesothelial cells (arrow) that was a contaminant in this transthoracic fine needle biopsy procedure. D: A different field from the same aspirate. Spindle cell carcinoid tumors may contain areas with morphology of a typical carcinoid tumor as depicted in this image.
Fig. 3.18: Transthoracic FNA of a Peripheral Spindle Cell Carcinoid Tumor. Note the tissue fragments of spindle cells with uniform nuclei containing typical salt-pepper chromatin.
Since the various neuroendocrine tumors of the lung share several of the morphologic features, their differential diagnostic possibilities are similar with some exceptions. In order to avoid repetition, the differential diagnoses of carcinoid tumors are discussed in the section on Small Cell Carcinoma (Table 3.3 and see Table 3.9).
METASTATIC CARCINOID TUMORS TO OTHER BODY SITES
Pulmonary carcinoid tumors or NECs grade I metastasize to other body sites infrequently as compared to higher grade NECs. Common sites for metastases are hilar/mediastinal lymph nodes, liver, bones, skin, and subcutaneous tissues (Figs. 3.25,3.26,3.27 and 3.28). The cytomorphology of the metastatic carcinoid tumors is usually characteristic enough for their correct identification.
TABLE 3.2. CYTOPATHOLOGIC FEATURES OF CARCINOID TUMOR, SPINDLE CELL TYPE
Cellularity
Variable, generally very cellular
Presentation
Loosely cohesive cells and in tissue fragments with fascicular pattern or swirls
Cells
Round to spindle shaped, well to poorly defined cell borders
Nucleus
Round to oval; oblong; smooth nuclear borders; N/C ratios generally high; chromatin coarsely granular, salt-pepper type; nucleolus +/-; no nuclear molding; no karyorrhexis; mitoses absent; no stretch artifacts
Cytoplasm
Scant to moderate; rarely oncocytic
Background
Clean
Histochemistry
Argyrophilic
Immunoprofile
Reactive to neuroendocrine markers and (CAM5, 2 and CK7), TTF-1, CD56
Differential Diagnoses of Spindle Cell Carcinoid Tumor (Figs. 3.19 and 3.20)
Fig. 3.19: A, B: FNA of a pulmonary nodule from a patient with a history of medullary thyroid carcinoma. Without the history, this neoplasm may be interpreted as a spindle cell carcinoid tumor.
Fig. 3.20: A, B: FNA of malignant melanoma with a spindle cell pattern. Note the similarity to spindle cell carcinoid tumor seen in Figure 3.17.
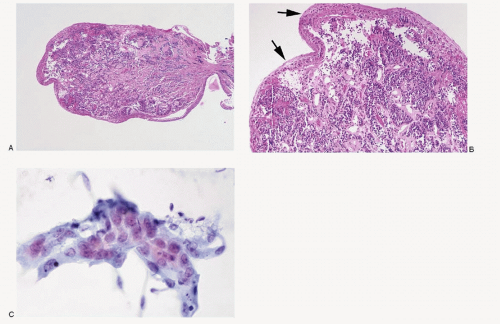
Fig. 3.21: A: Histologic section of a bronchial biopsy with a submucosal tumor proven to be a carcinoid tumor (low power, H&E). B: Higher magnification shows the overlying epithelium with squamous metaplasia with significant atypia (arrows) (medium power, H&E). C: Bronchial brushings showing a tissue fragment of atypical squamous epithelium. No neoplastic cells indicative of a carcinoid tumor were identified. The carcinoid tumor being submucosal with an intact overlying mucosa does not yield to the brush, resulting in a false-negative diagnosis.
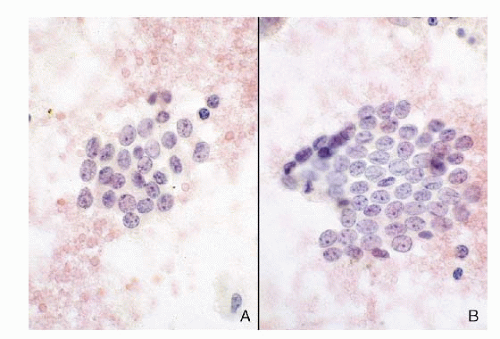
Fig. 3.22: FNA of a Lung Mass. The aspirate was poorly cellular. A: This field shows a small number of dispersed cells, which were misinterpreted as lymphocytes. B: Another field revealed a tissue fragment of uniform cells that closely resembles a mesothelium. The surgically excised tumor was proven to be a typical carcinoid tumor.
TABLE 3.3 DIFFERENTIAL DIAGNOSES OF TYPICAL CARCINOID TUMOR
1. Lymphocytes from nonneoplastic lymphoproliferative disorders
8. Poorly differentiated squamous carcinoma and basaloid variant
9. Poorly differentiated adenocarcinoma; primary or metastatic
10. Adenoid cystic carcinoma
11. Malignant lymphoma
12. Thymoma
13. Thymic carcinoma
14. Thymic carcinoid
15. Malignant melanoma
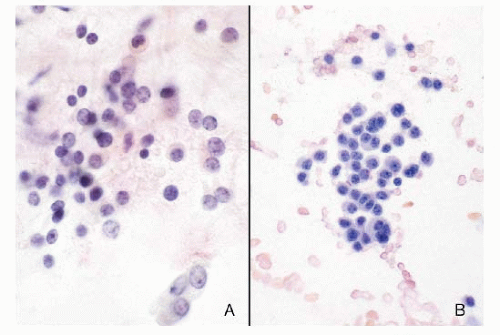
Fig. 3.23: A, B: Another example of a poorly cellular sample, resulting in a false-negative diagnosis. The neoplastic cells are few, discrete, resembling lymphoid cells, and interpreted as such. Surgical excision confirmed a carcinoid tumor.
Atypical carcinoid tumors are uncommon neoplasms, behave more aggressively than the typical carcinoid tumors, and comprise 11% to 24% of all pulmonary carcinoids. They are more frequent in males, occurring at an older age than typical carcinoid tumors. Roughly 20% of the cases demonstrate metastasis at the time of presentation, with regional lymph node involvement in 40% to 48% of the cases. Five-year survival is reported to be 69%.
GROSS AND HISTOLOGIC FEATURES
Grossly, atypical carcinoid tumors tend to be larger than the typical carcinoids and may reveal areas of hemorrhage and necrosis.
Microscopically, atypical carcinoids show a spectrum of findings that range from patterns resembling a typical carcinoid to one that appears very similar to small cell carcinoma.
Histologic diagnosis of atypical carcinoid is based on the presence of one or more of the following four criteria: (1) increased number of mitotic figures; (2) pleomor-phism or irregularity of the nuclei, prominent nucleoli, hyperchromasia, and increased N/C ratios; (3) areas of increased cellularity with disorganization of the architecture; and (4) necrosis either punctate, focal, or large areas (Fig. 3.29). Except for cytologic atypia, features such as punctate necrosis, mitotic rate, and invasive characteristics cannot be appreciated in cytologic preparations.
Differential Diagnoses of Typical Carcinoid Tumor
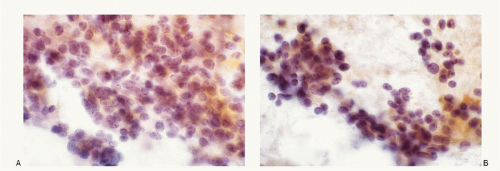
Fig. 3.24: A, B: Carcinoid tumor cells in bronchial brushings. Note coarsely granular nuclear chromatin. C: Pulmonary adenocarcinoma in a respiratory specimen. D: Pulmonary adenocarcinoma in FNA. Note the similarity between carcinoid tumor cells (see Fig. 3.13) and adenocarcinoma cells, when the latter are of small size.
Fig. 3.25: A-D: Metastatic Carcinoid Tumor. FNA of a subcutaneous mass over the shoulder in a patient with a history of pulmonary carcinoid tumor.
Fig. 3.26: Metastatic Pulmonary Carcinoid Tumor in Liver. A: FNA of a liver mass in a patient with a history of pulmonary carcinoid tumor (same case as Fig. 3.4). B: Another example of a metastatic pulmonary carcinoid to the liver. FNA of one of the multiple liver nodules with typical cytomorphology of carcinoid tumor.
Fig. 3.27: Metastatic Pulmonary Carcinoid Tumor in Serous Effusion Fluid. This syncytial tissue fragment of neoplastic cells shows morphology that is suggestive of an adenocarcinoma. The patient had a history of carcinoid tumor of the lung with resection.
Fig. 3.28: A, B: Metastatic Carcinoid Tumor in Bone. FNA of a lytic lesion of the bone in a patient with a history of pulmonary carcinoid tumor. The aspirate was very cellular, consisting of several syncytial tissue fragments, consisting of uniform round cells with high N/C ratios, and scant to indistinct cytoplasm. There is no nuclear molding, karyorrhexis or necrosis. Immunostains on the cell block confirmed neuroendocrine nature.
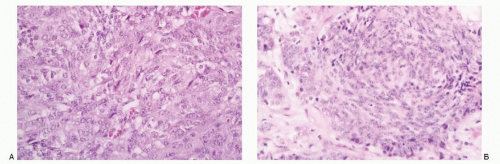
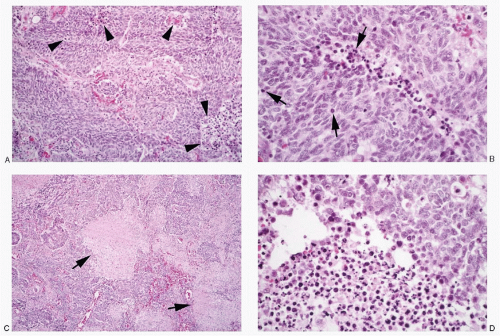
Fig. 3.29: Histologic Features of Atypical Carcinoid Tumor. A: This carcinoid tumor composed of a mixed spindle and round cell pattern shows punctate necrosis (arrowheads) (H&E). B: Higher magnification of (A). Also note occasional mitosis (arrows) (H&E). C: This atypical carcinoid tumor shows large areas of necrosis (arrows) (H&E). D: Higher magnification of (C) highlighting the necrotic foci (H&E).
CYTOPATHOLOGIC FEATURES OF PULMONARY ATYPICAL CARCINOID TUMORS
The exact cytologic typing of an atypical carcinoid is not possible. Its cytologic interpretation ranges from a typical carcinoid to a small cell carcinoma (Table 3.4, Figs. 3.30,3.31,3.32,3.33 and 3.34). When tumor cell necrosis is minimal, mitotic figures are sparse, and the overall architecture is maintained, the cytologic pattern strongly resembles that of a typical carcinoid tumor (Fig. 3.30). With prominent nuclear atypia, mitosis, and necrosis, the cytologic pattern resembles either a small cell carcinoma or an LCNEC (Figs. 3.31,3.32,3.33 and 3.34). There is not a single cytologic feature that is characteristic of an atypical carcinoid tumor. The immunoprofile and the ultrastructural findings are similar to that of typical carcinoid tumors.
DIAGNOSTIC ACCURACY AND DIFFERENTIAL DIAGNOSES OF PULMONARY ATYPICAL CARCINOID TUMORS
As noted earlier, atypical carcinoid is a histologic diagnosis. It cannot be specifically typed accurately from cytologic samples. However, the general diagnosis of a neuroendocrine tumor can be easily made, but the diagnostic specificity is low. The differential diagnoses of atypical carcinoid tumors are the same as for other pulmonary neuroendocrine tumors (see Tables 3.3, 3.8,3.9 and 3.10).
TABLE 3.4. CYTOPATHOLOGIC FEATURES OF ATYPICAL CARCINOID
Cellularity
Variable, generally very cellular
Presentation
Cells dispersed, isolated, in loosely cohesive groups, or in syncytial tissue fragments as cords, nests, or anastomosing ribbons, occasional acinar pattern or rosettes; perivascular arrangement of cells in fine needle aspirates
Cells
Small, round to cuboidal; well to poorly defined cell borders; high N/C ratios; uniform to varying degrees of pleomorphism
Nucleus
Round to oval with smooth nuclear membrane; salt-pepper chromatin pattern and inconspicuous nucleoli to hyperchromatic nuclei with nuclear molding and nucleoli; mitoses +/-; karyorrhexis +/-
Cytoplasm
Variable, scant insignificant to moderate amount
Background
Clean to necrosis
Histochemistry
Argyrophilic
Immunoprofile
Reactive to neuroendocrine markers and cytokeratin (CAM5, 2 and CK7), TTF-1, CD56
Ultrastructure
Membrane-bound neurosecretory granules
Modified from Kini SR. Color Atlas of Pulmonary Cytopathology. New York: Springer-Verlag Inc.; 2002.
Only gold members can continue reading. Log In or Register to continue