|
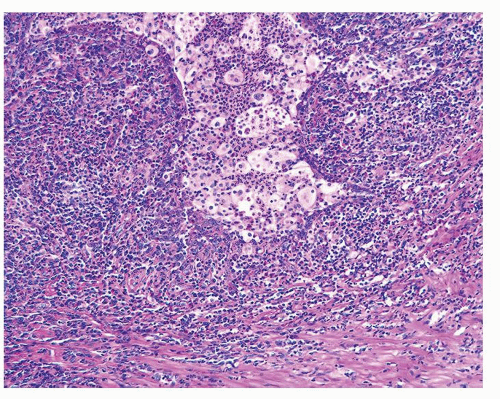 Figure 1.1.1 Early lesion of NSGP. |
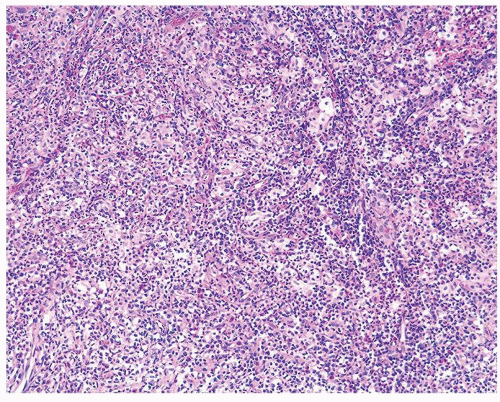 Figure 1.1.2 NSGP with destruction of acini by polymorphous infiltrate. |
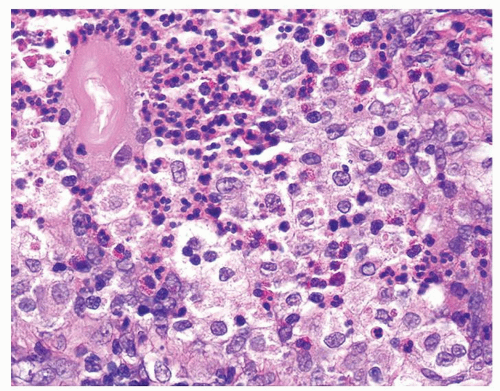 Figure 1.1.3 Central area of NSGP with microabscess formation, yet lacking caseation. In addition to neutrophils, there are histiocytes, lymphocytes, and eosinophils. |
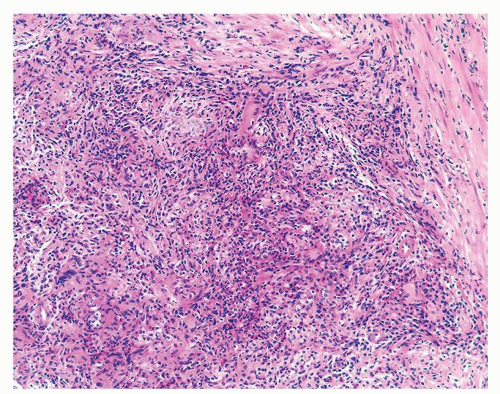 Figure 1.1.4 Lobular infiltrate of NSGP. |
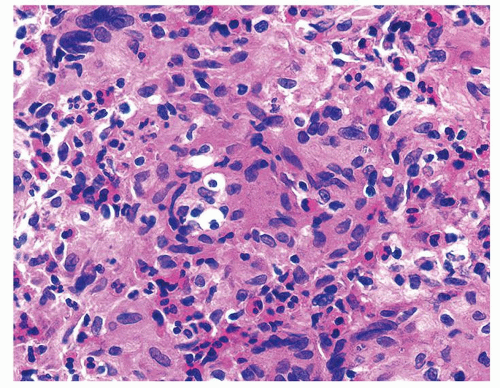 Figure 1.1.5 NSGP with more histiocytes, yet admixed eosinophils and neutrophils more typical of NSGP than of infectious granuloma. |
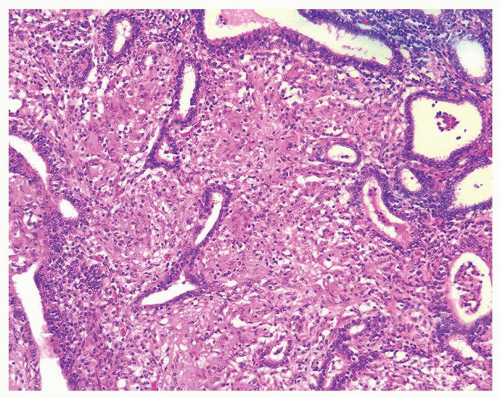 Figure 1.1.6 Infectious granuloma with periglandular granulomas consisting of histiocytes and lymphocytes without admixed plasma cells, neutrophils, or eosinophils. |
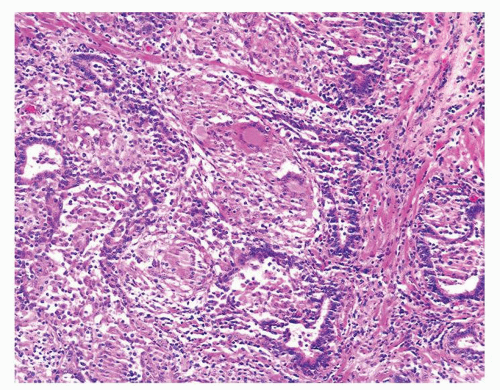 Figure 1.1.7 Infectious granuloma containing multinucleated giant cells surrounding intact glands. |
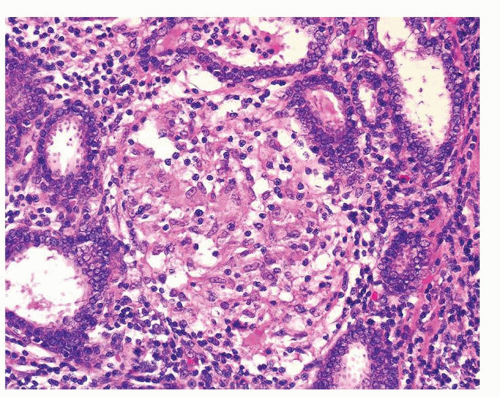 Figure 1.1.8 Higher magnification of infectious granuloma with intact glands. |
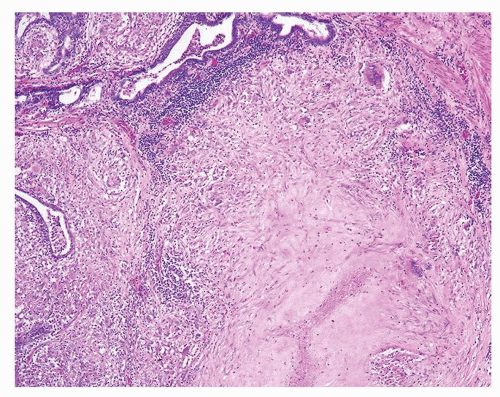 Figure 1.1.9 Infectious granuloma with focal intact glands (left) and larger granulomas (center) that have destroyed glands. |
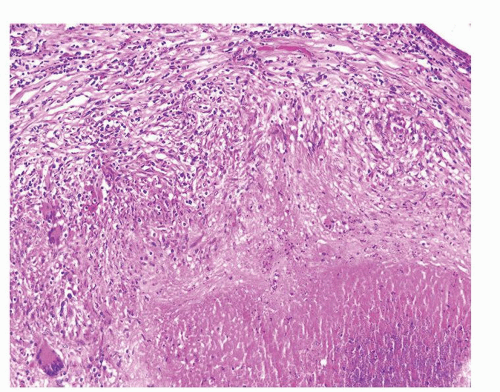 Figure 1.1.10 Infectious granuloma with caseous necrosis (bottom). |
|
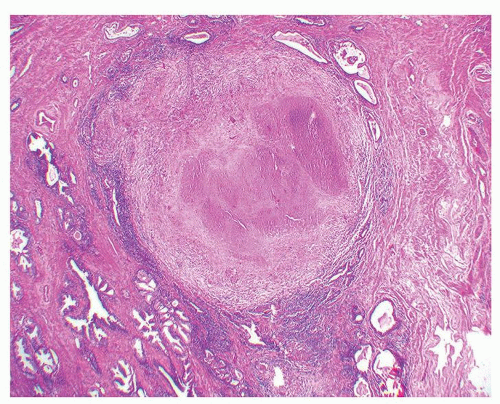 Figure 1.2.1 Infectious necrotizing granuloma with relative sparing of glands. |
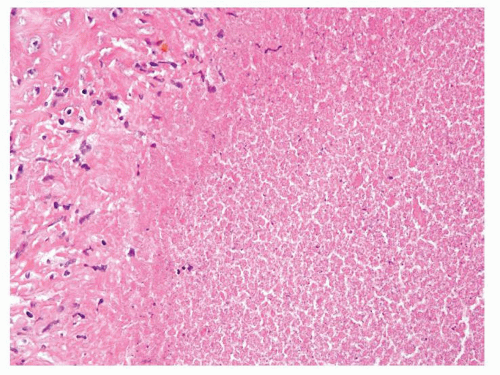 Figure 1.2.2 Caseous necrosis with fine granular debris surrounded by histiocytes. |
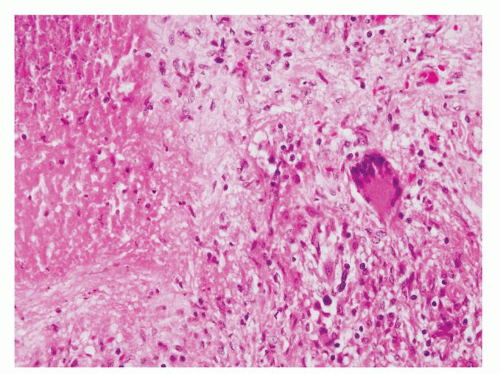 Figure 1.2.3 Caseous necrosis (left) with adjacent multinucleated histiocytes. |
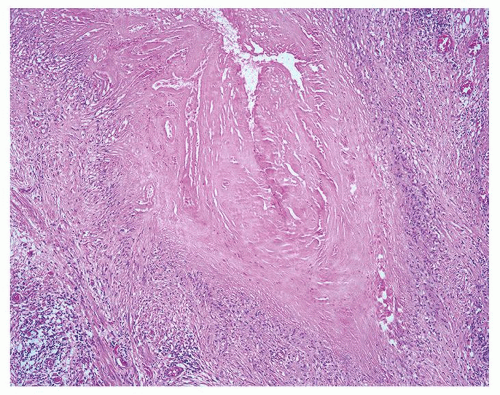 Figure 1.2.4 Oval-shaped postbiopsy granuloma with central necrosis. |
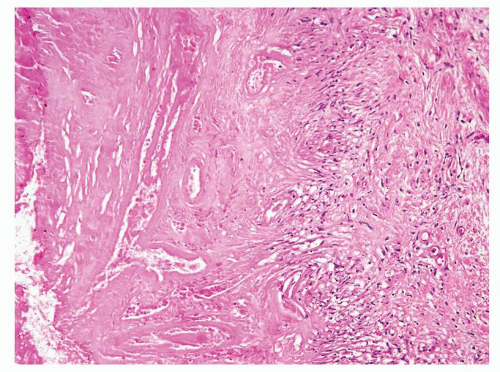 Figure 1.2.5 Postbiopsy granuloma with necrobiotic center with ghosts of necrotic vessels. |
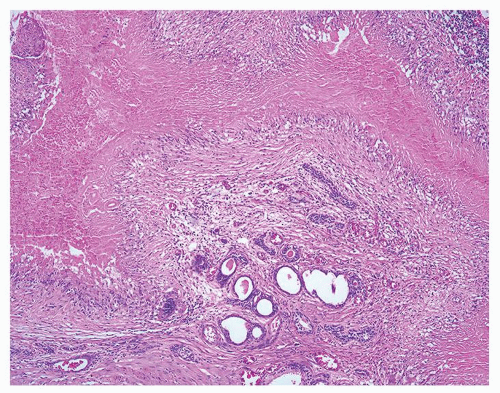 Figure 1.2.6 Irregular linear necrobiotic granuloma of postbiopsy granuloma. |
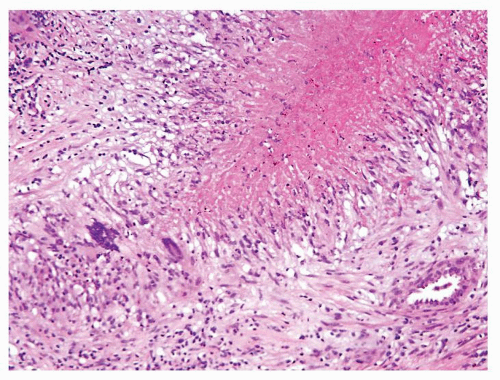 Figure 1.2.7 Postbiopsy ovoid granuloma mimicking an infectious granuloma with palisading histiocytes and scattered multinucleated histiocytes. |
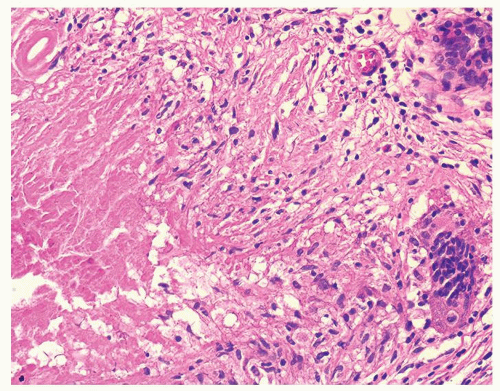 Figure 1.2.8 Higher magnification of Figure 1.2.7 with central necrosis lacking the fine granular amorphous appearance of infectious granulomas. |
|
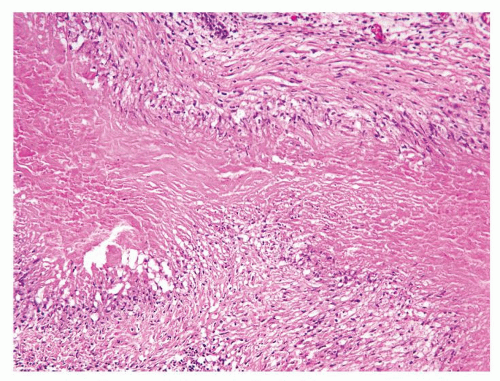 Figure 1.3.1 Linear necrobiotic postbiopsy granuloma with palisading histiocytes. |
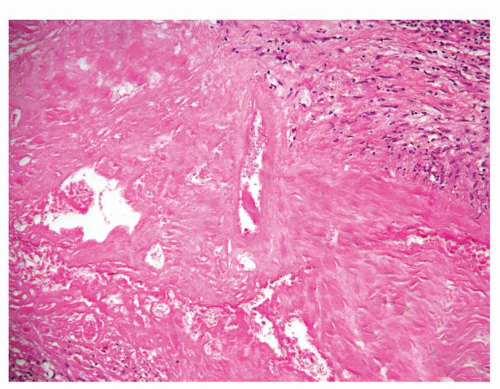 Figure 1.3.2 Postbiopsy granuloma ghost of blood vessels. |
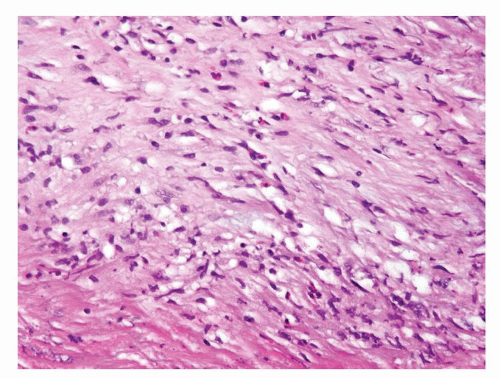 Figure 1.3.3 Scattered eosinophils (top) surrounding postbiopsy granuloma. |
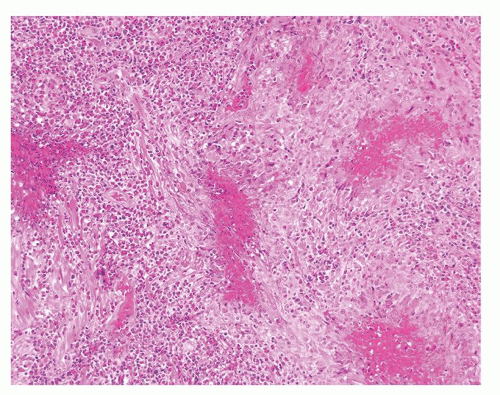 Figure 1.3.4 Allergic granuloma with multiple relatively uniformly sized and shaped ovoid necrotic granulomas. |
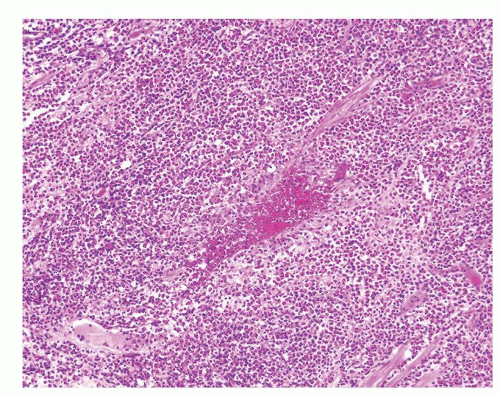 Figure 1.3.5 Allergic granuloma central eosinophilic necrosis surrounded by histiocytes and numerous eosinophils. |
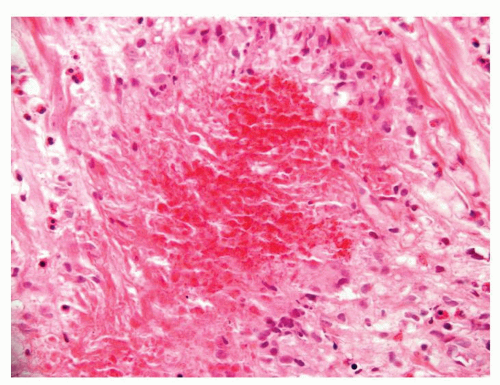 Figure 1.3.6 Central necrosis of allergic granuloma lacking necrotic prostate structures. |
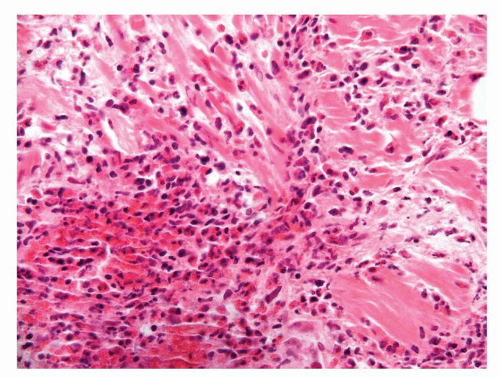 Figure 1.3.7 Allergic granuloma necrosis surrounded by numerous eosinophils. |
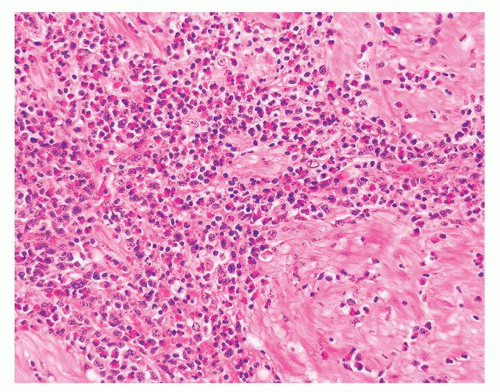 Figure 1.3.8 Numerous eosinophils of allergic granuloma infiltrating prostatic stroma. |
|
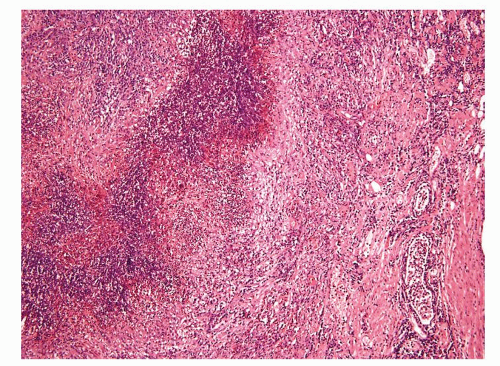 Figure 1.4.1 Abscess formation in acute prostatitis. |
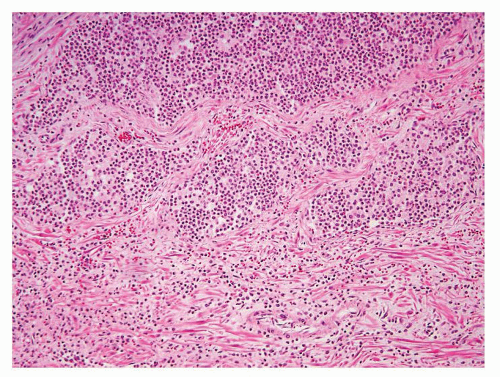 Figure 1.4.2 Sheets of neutrophils with acute prostatitis. |
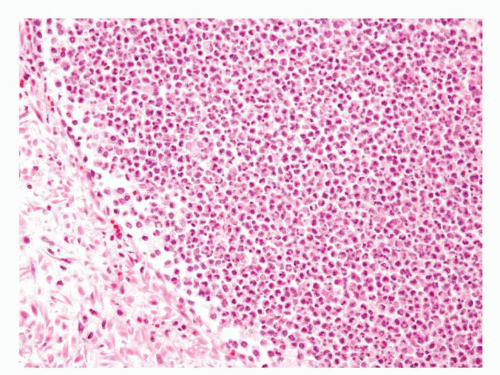 Figure 1.4.3 Higher magnification of Figure 1.4.2 with abscess formation. |
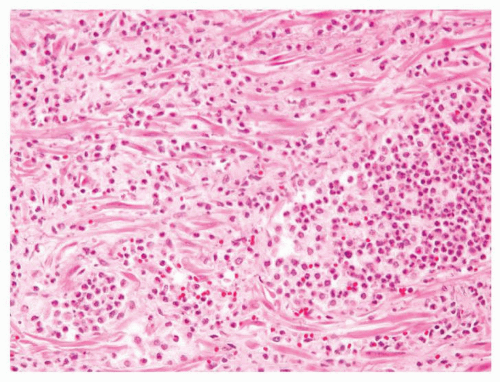 Figure 1.4.4 Diffuse infiltration of stroma by neutrophils in acute prostatitis. |
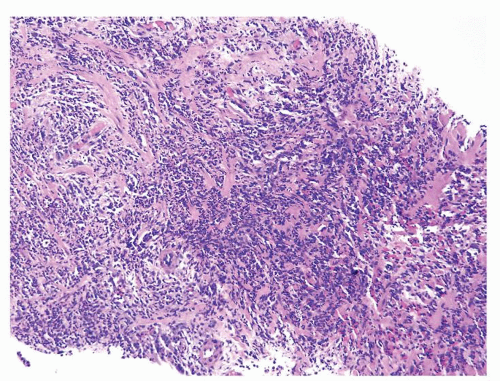 Figure 1.4.5 Low magnification of acute prostatitis with heavily inflamed prostatic stroma. |
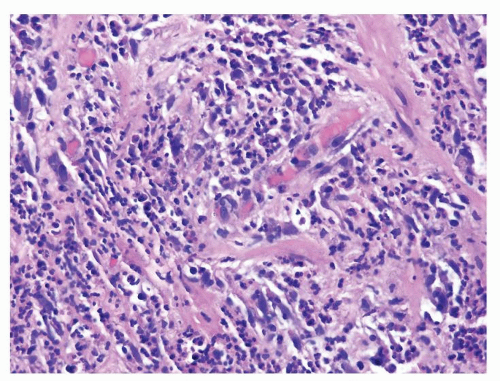 Figure 1.4.6 Higher magnification of Figure 1.4.5 showing numerous neutrophils infiltrating prostatic stroma. |
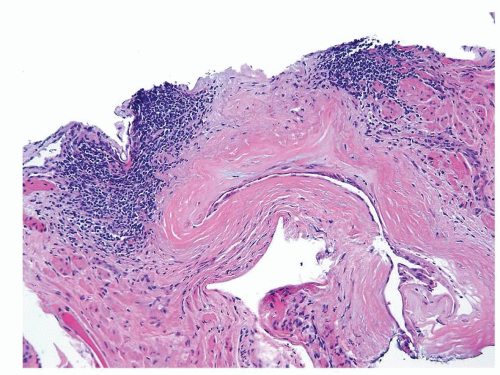 Figure 1.4.7 Nonspecific periglandular chronic inflammation. |
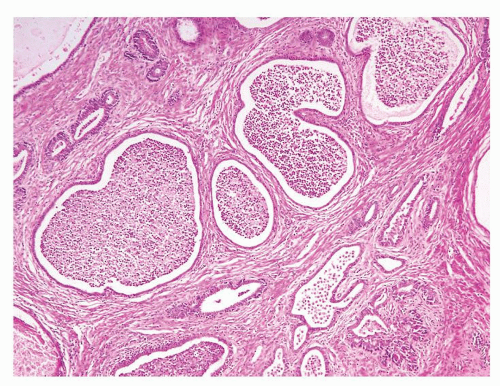 Figure 1.4.8 Nonspecific acute inflammation in prostate glands. |
|
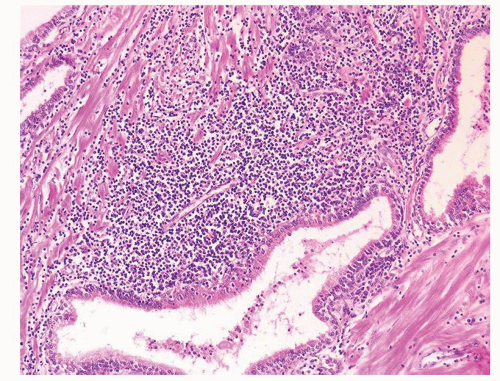 Figure 1.5.1 Focal periglandular nonspecific chronic inflammation. |
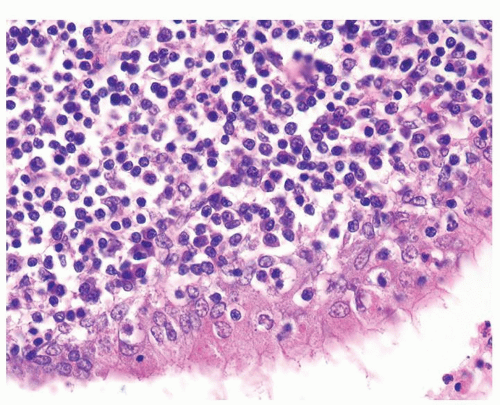 Figure 1.5.2 Higher magnification of Figure 1.5.1 with lymphocytes and plasma cells. |
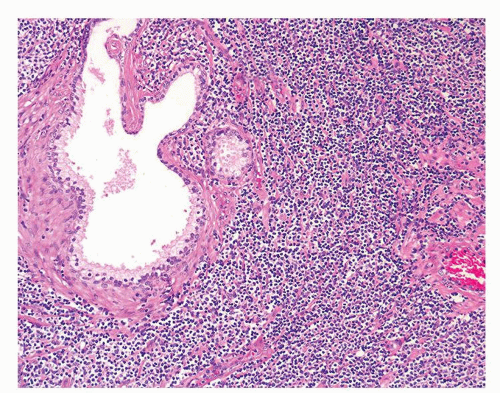 Figure 1.5.3 Extensive periglandular lymphocytic infiltrate of CLL. |
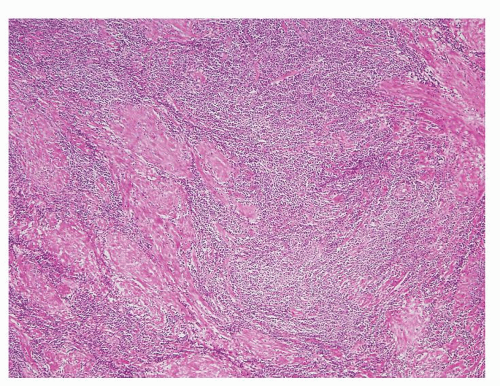 Figure 1.5.4 Moderately dense lymphocytic infiltrate of CLL extending into stroma. |
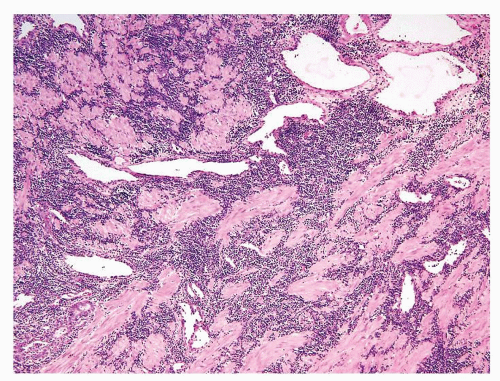 Figure 1.5.5 CLL with dense infiltrate extensively involving prostatic stroma. |
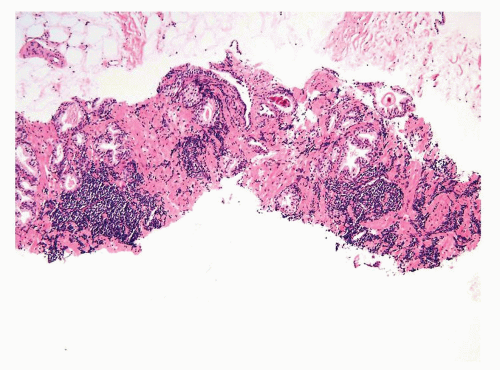 Figure 1.5.6 Needle biopsy with scattered dense infiltrates of CLL not in a periglandular distribution. |
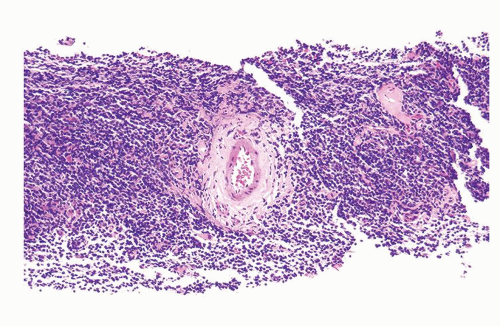 Figure 1.5.7 CLL with effacement of prostate by dense lymphoid infiltrate. |
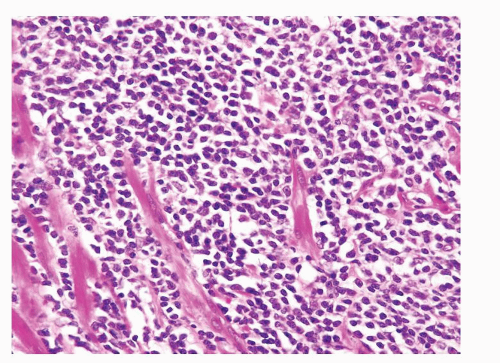 Figure 1.5.8 Monotonous CLL lymphocytic infiltrate. |
|
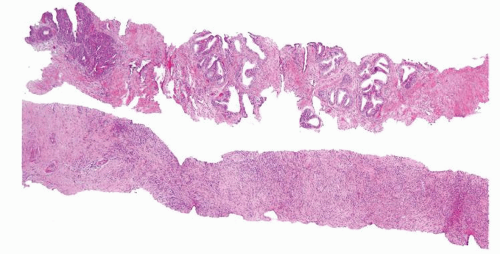 Figure 1.6.1 NSGP at low magnification (bottom core) can extensively involve a core destroying underlying benign glands and stroma, mimicking carcinoma. |
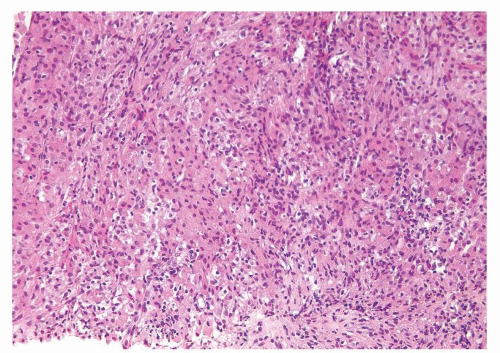 Figure 1.6.2 Low magnification of NSGP with sheets of epithelioid cells. |
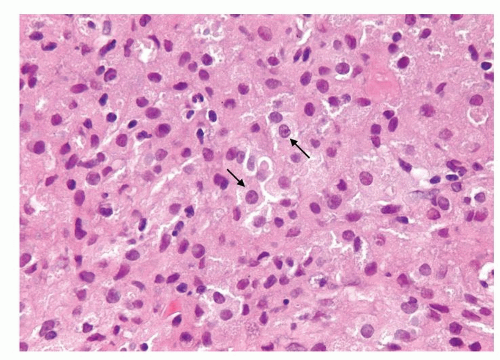 Figure 1.6.3 Higher magnification of Figure 1.6.2 with epithelioid histiocytes having prominent nucleoli (arrows). |
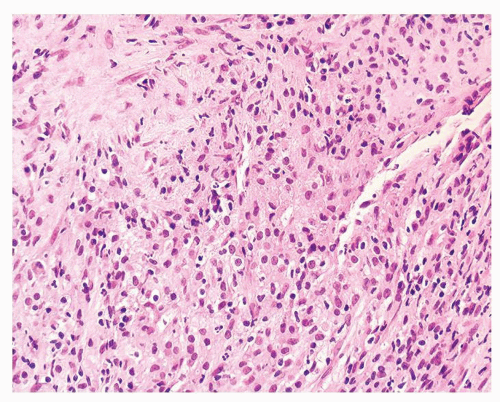 Figure 1.6.4 Low magnification of NSGP with sheets of epithelioid cells. |
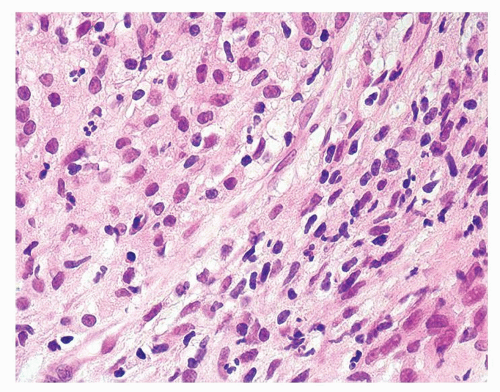 Figure 1.6.5 Higher magnification of histiocytes and admixed neutrophils and lymphocytes. |
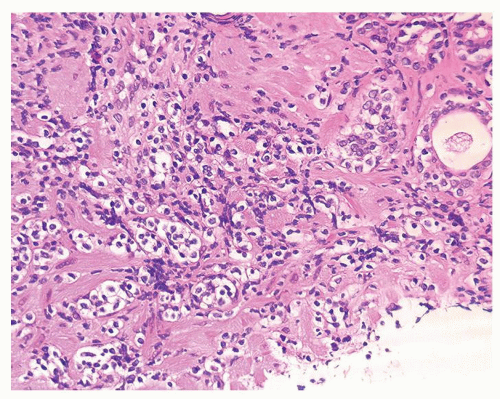 Figure 1.6.6 Low magnification of NSGP with cords of epithelioid cells. |
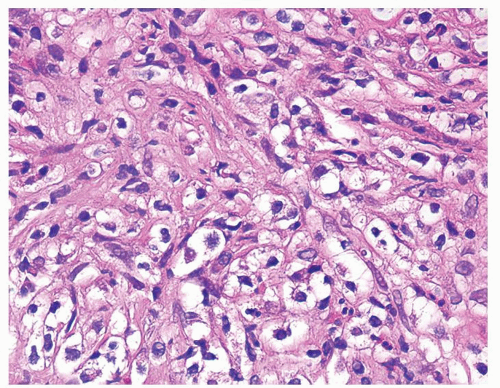 Figure 1.6.7 Higher magnification of Figure 1.6.6 with epithelioid histiocytes and admixed neutrophils and lymphocytes. |
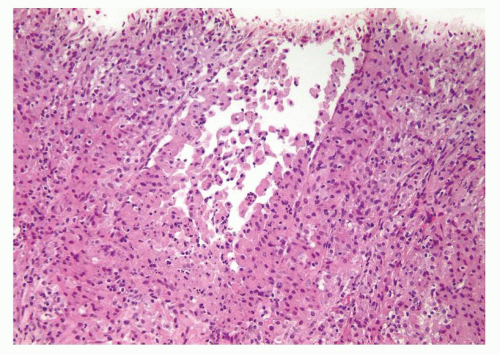 Figure 1.6.8 Partially ruptured dilated prostatic gland with intraluminal and periglandular epithelioid histiocytes. |
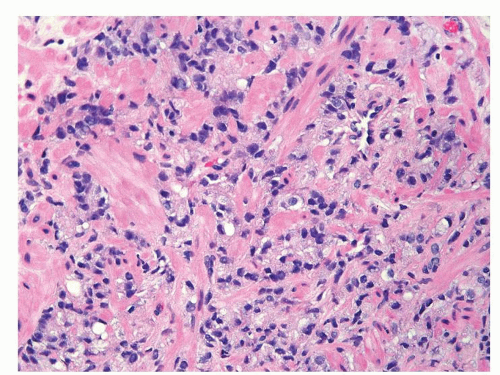 Figure 1.6.9 Cords of infiltrating relatively bland Gleason score 10 adenocarcinoma without admixed inflammation. |
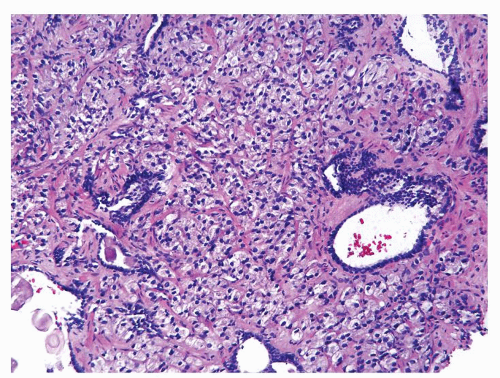 Figure 1.6.10 Gleason score 10 adenocarcinoma with foamy cytoplasm mimicking histiocytes, yet lacking interspersed inflammation. |
|
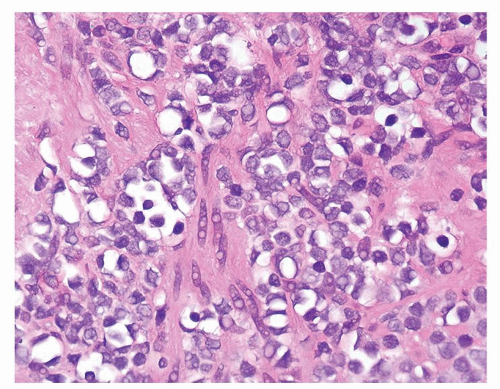 Figure 1.7.1 Bland lymphocytes with some having eccentric vacuoles. |
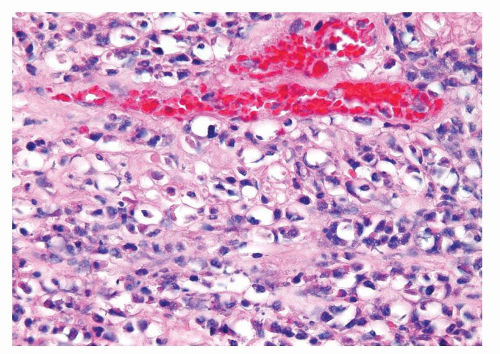 Figure 1.7.2 Lymphocytes with most having a centrally located nucleus surrounded by a clear space. |
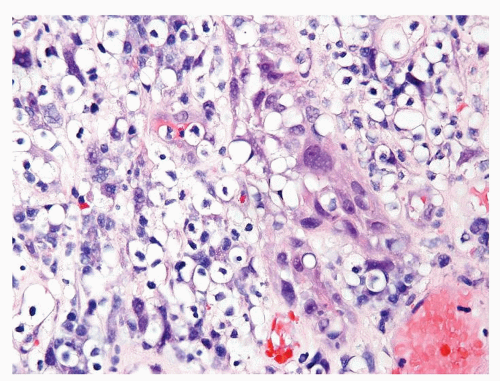 Figure 1.7.3 Vacuolated lymphocytes. |
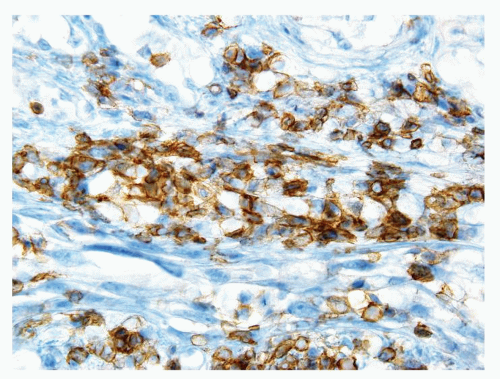 Figure 1.7.4 CD20 staining of signet-ring cell lymphocytes (same case as Fig. 1.7.3). |
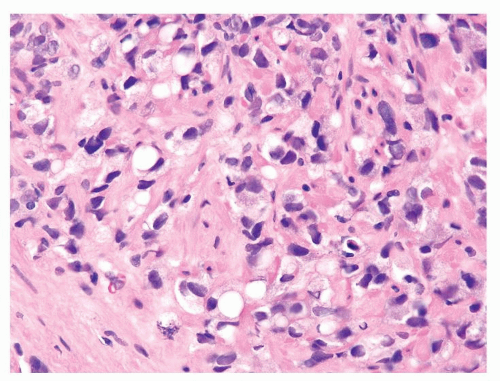 Figure 1.7.5 Gleason score 10 adenocarcinoma with vacuoles. Nuclei are more variably shaped, hyperchromatic, and larger than of lymphocytes. |
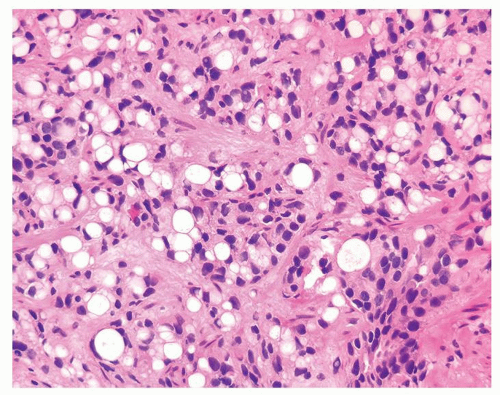 Figure 1.7.6 Extensive signet-ring cell-like change in adenocarcinoma with hyperchromatic nuclei. |
|
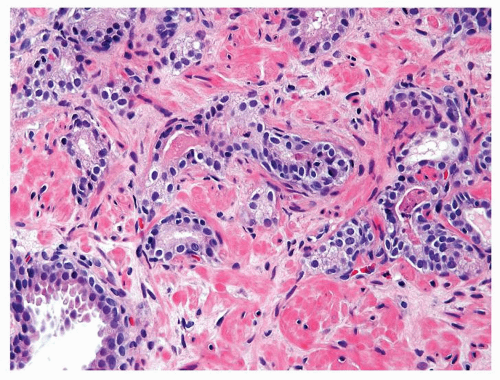 Figure 1.8.1 Crowded benign glands with intraluminal acute inflammation (right). |
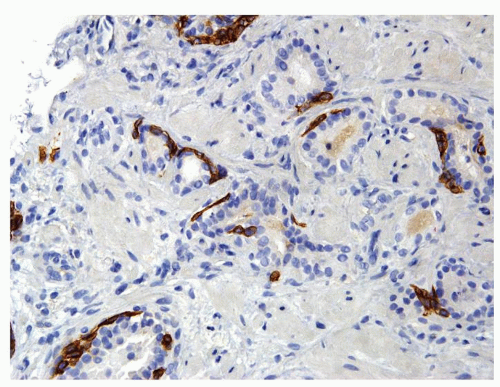 Figure 1.8.2 Same case as Figure 1.8.1 with a patchy basal cell layer for high molecular weight cytokeratin ruling out carcinoma. |
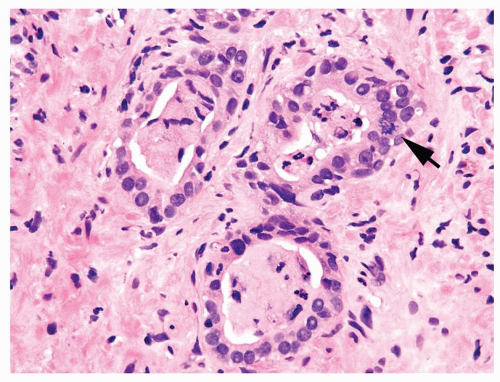 Figure 1.8.3 Benign atrophic glands with acute inflammation, nucleoli, and mitotic figure (arrow). |
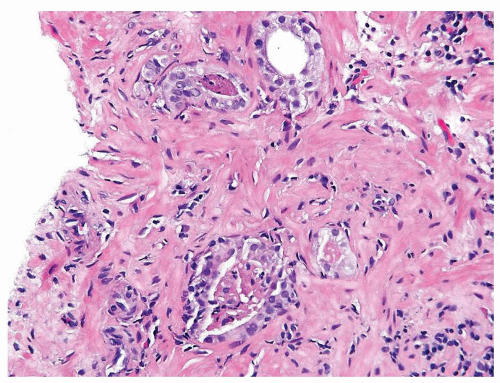 Figure 1.8.4 Cluster of crowded glands suspicious for carcinoma, yet a definitive diagnosis cannot be made due to associated inflammation. |
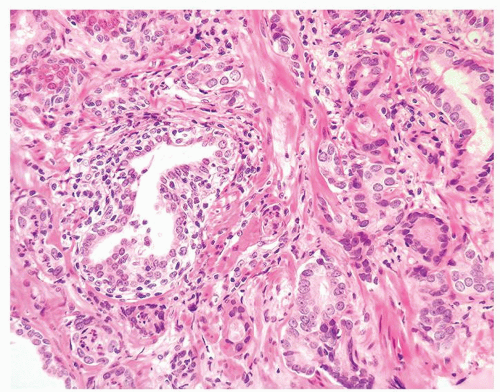 Figure 1.8.5 Small atypical glands of carcinoma associated with a lymphocytic infiltrate around benign gland (left). |
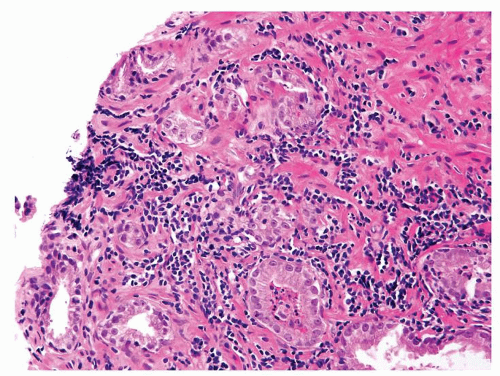 Figure 1.8.6 Glands with huge nucleoli are associated both with heavily inflamed glands (lower) as well as similarly atypical glands (upper) with less inflammation, the latter diagnostic of carcinoma. |
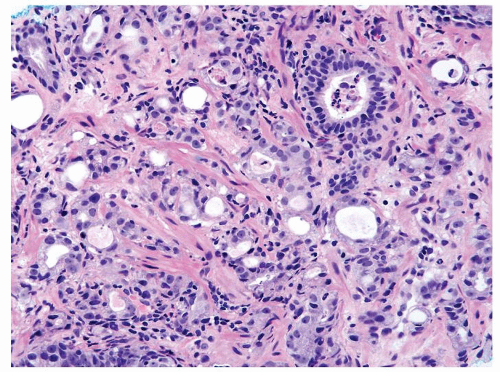 Figure 1.8.7 Inflamed cancer with greater degree of cytologically atypia compared to adjacent benign inflamed gland (upper right). |
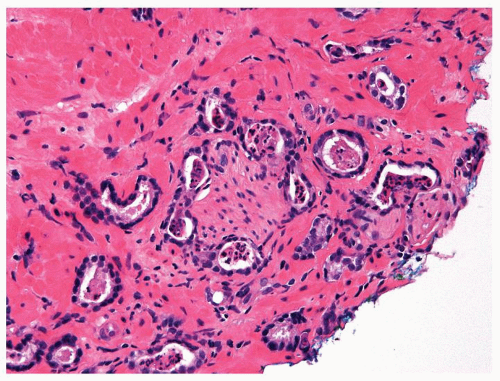 Figure 1.8.8 Perineural invasion by inflamed carcinoma glands. |
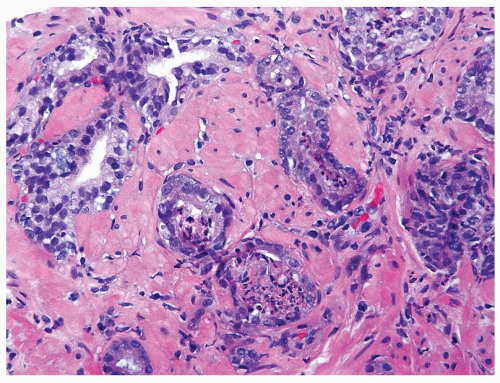 Figure 1.8.9 Adenocarcinoma with inflammation. |
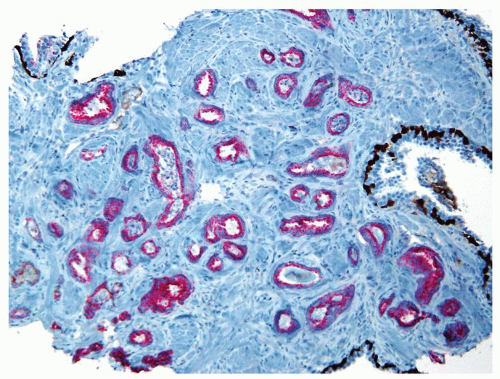 Figure 1.8.10 Same case as Figure 1.8.9 with numerous inflamed atypical glands negative for p63 and high molecular weight cytokeratin (brown) and positive for AMACR (red), consistent with carcinoma. |
|
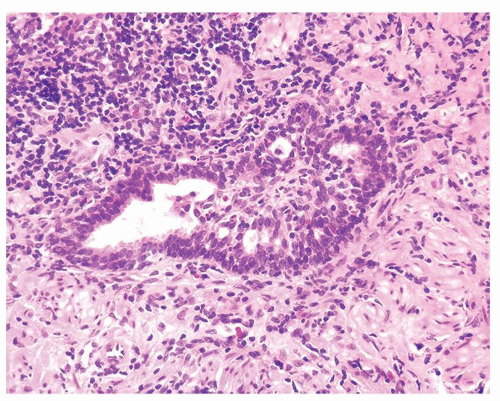 Figure 1.9.1 Partially involved inflamed benign gland with cribriform pattern. Nuclei have a slightly spindled appearance. |
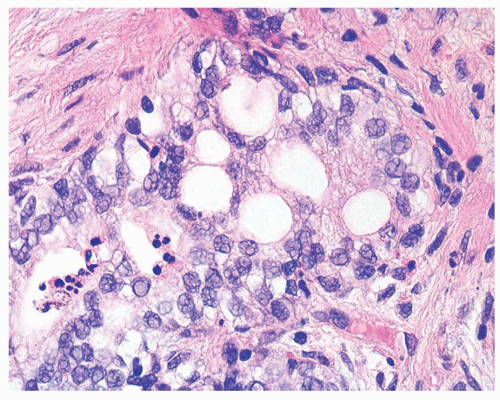 Figure 1.9.2 Inflamed benign cribriform gland with intraluminal acute inflammation. Nuclei are enlarged with visible nucleoli yet lack nuclear hyperchromasia. |
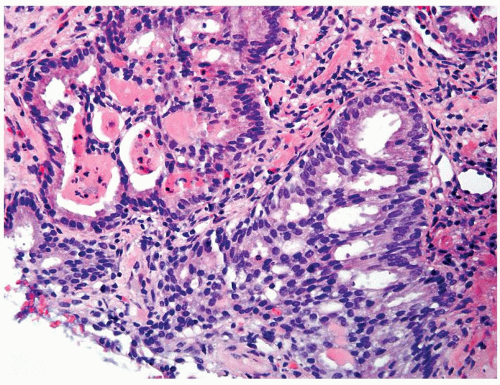 Figure 1.9.3 Inflamed benign cribriform gland with intraluminal acute inflammation. |
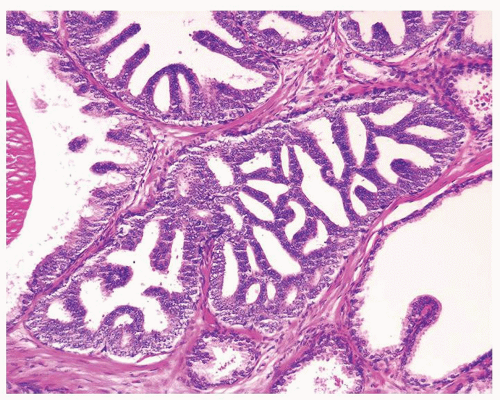 Figure 1.9.4 Cribriform high-grade PIN with rigid transluminal bridges, lacking associated inflammation. |
|
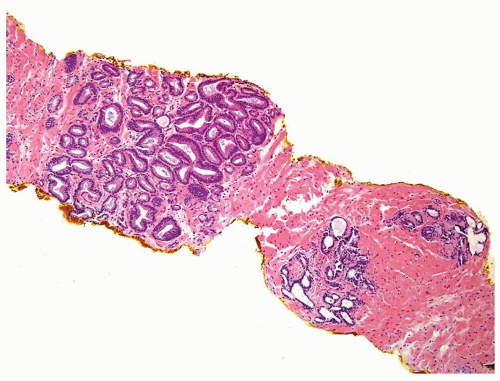 Figure 1.10.1 Benign atrophic glands (lower right) with very basophilic appearance compared to adenocarcinoma with amphophilic cytoplasm (upper left). |
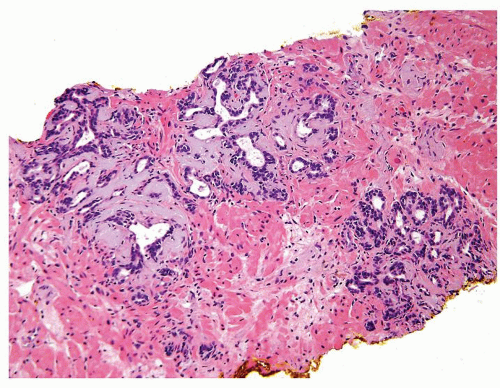 Figure 1.10.2 Lobular collections of rounded basophilic glands. |
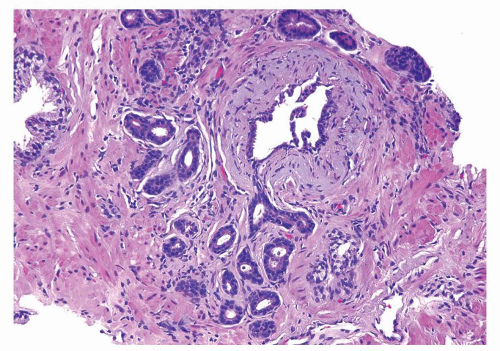 Figure 1.10.3 Post-atrophic hyperplasia with central dilated glands and surrounding smaller atrophic glands. |
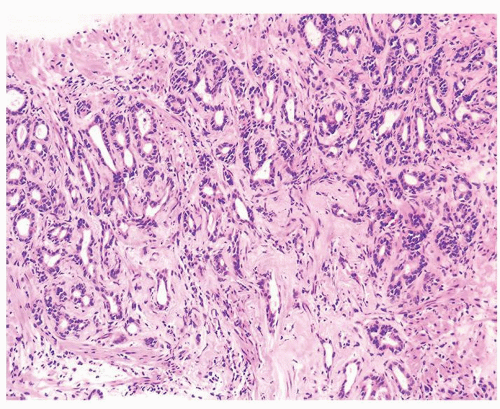 Figure 1.10.4 Post-atrophic hyperplasia with sclerosis imparting an infiltrative pattern on needle biopsy where the entire lesion is not visualized. |
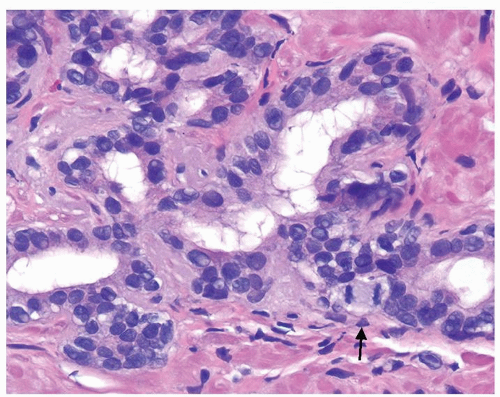 Figure 1.10.5 Post-atrophic hyperplasia showing occasional nucleoli and mitotic figure (arrow). |
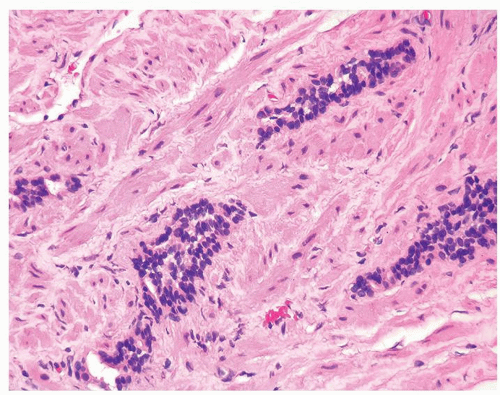 Figure 1.10.6 Tangential section of PAH with columns composed of cells with bland, small nuclei and scant cytoplasm. |
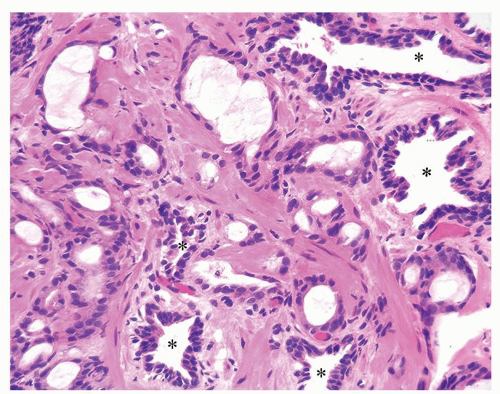 Figure 1.10.7 Small glands of atrophic adenocarcinoma infiltrating between larger benign glands with luminal undulations (asterisk). |
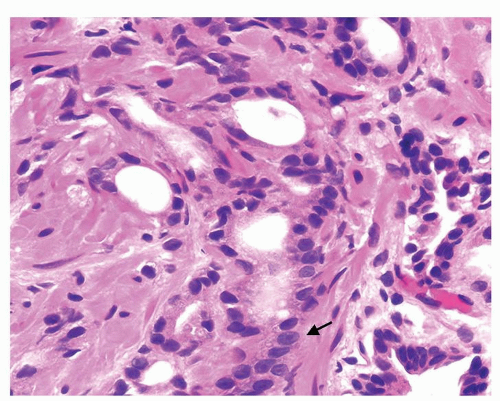 Figure 1.10.8 Higher magnification of Figure 1.10.7 showing some of the small atrophic glands of adenocarcinoma with prominent nucleoli (arrow). |
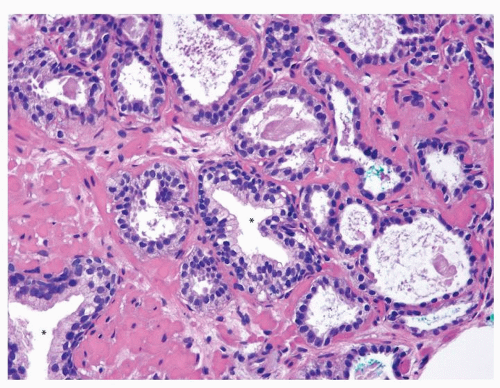 Figure 1.10.9 Atrophic adenocarcinoma infiltrating between two benign glands (asterisk). |
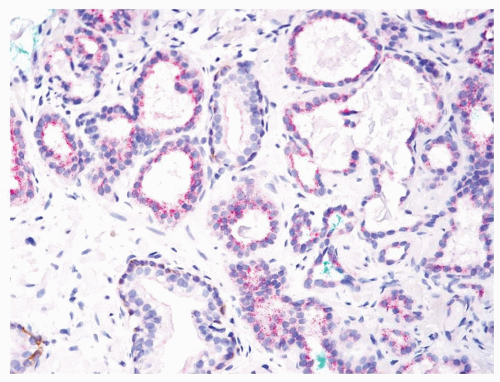 Figure 1.10.10 Triple stain of Figure 1.10.9 with atrophic adenocarcinoma lacking basal cells (brown) and positive for AMACR (red). |
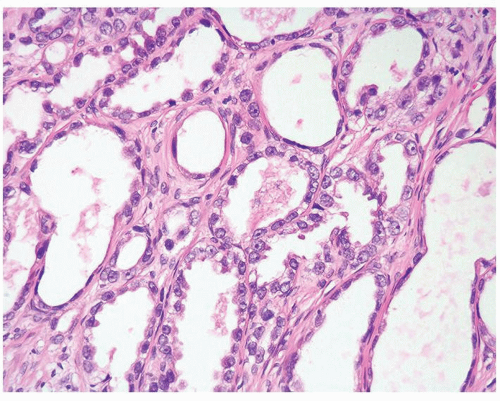 Figure 1.10.11 Atrophic adenocarcinoma with diffuse very prominent nucleoli. |
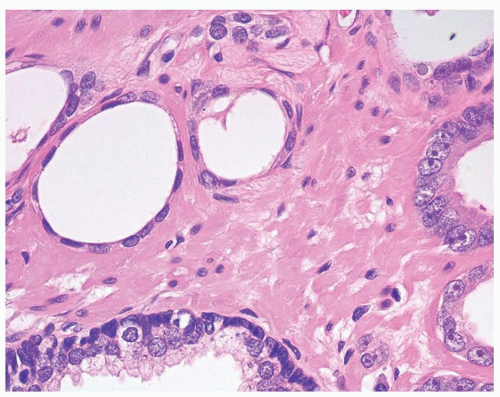 Figure 1.10.12 Atrophic adenocarcinoma showing a spectrum of nuclear atypia from none (left) to focal moderate (center) to marked (right) where the glands begin having slightly more cytoplasm. |
|
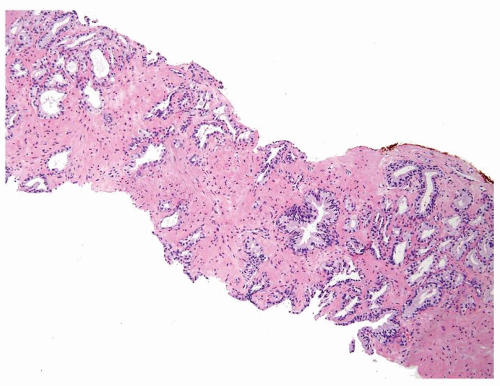 Figure 1.11.1 Multiple foci of partial atrophy on needle biopsy. |
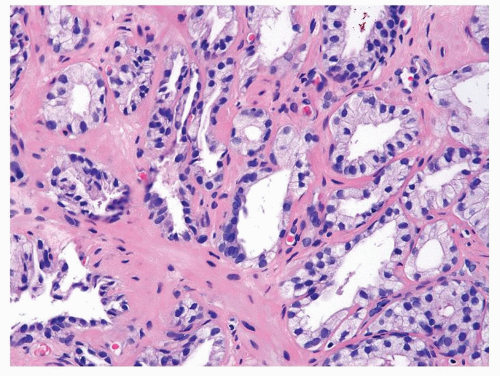 Figure 1.11.2 Higher magnification of Figure 1.11.1. |
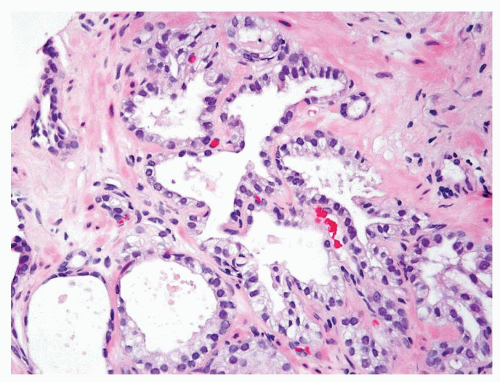 Figure 1.11.3 Partial atrophy with several glands having luminal undulation. |
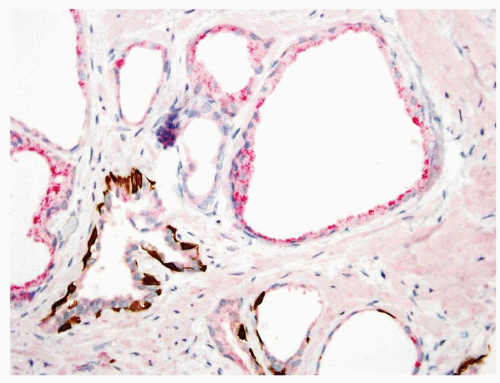 Figure 1.11.4 Triple stain of Figure 1.11.3 with several glands of partial atrophy having a patchy basal cell layer (bottom) with others negative for basal cells and positive for AMACR (top). |
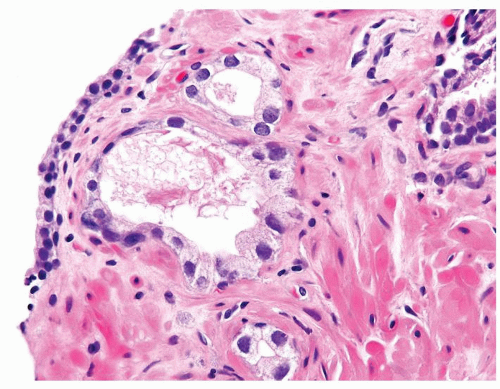 Figure 1.11.5 Partial atrophy with slightly enlarged nuclei. |
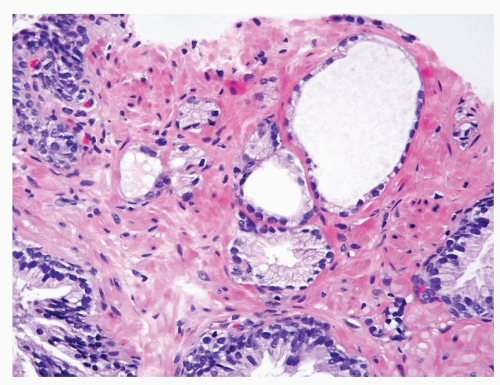 Figure 1.11.6 Partial atrophic glands admixed with some benign glands having more abundant cytoplasm. |
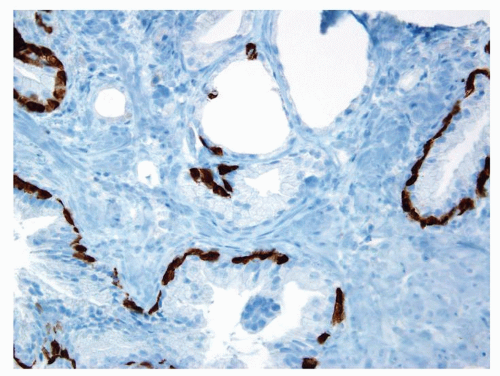 Figure 1.11.7 Some of the partially atrophic glands have patchy basal cells with others lacking high molecular weight cytokeratin staining. |
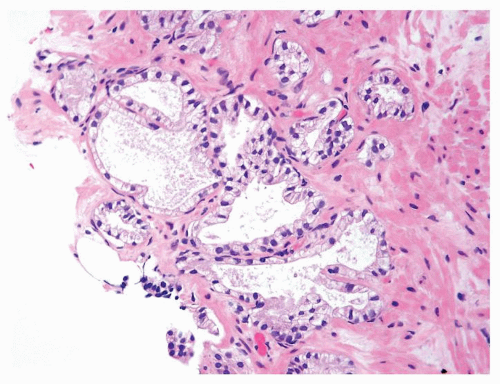 Figure 1.11.8 Classic example of partial atrophy. |
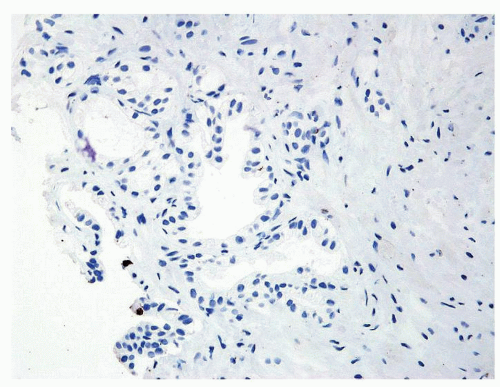 Figure 1.11.9 Partial atrophy negative for high molecular weight cytokeratin. |
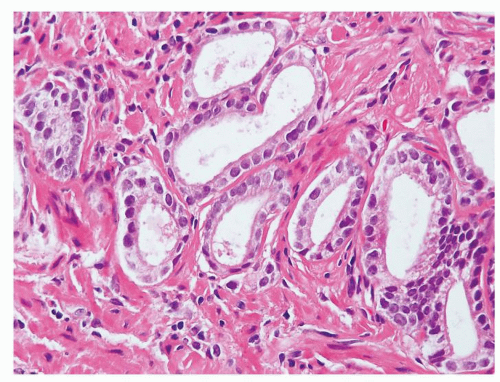 Figure 1.11.10 Adenocarcioma where malignant glands have straight luminal borders, slightly more apical cytoplasm, and numerous prominent nucleoli. |
|
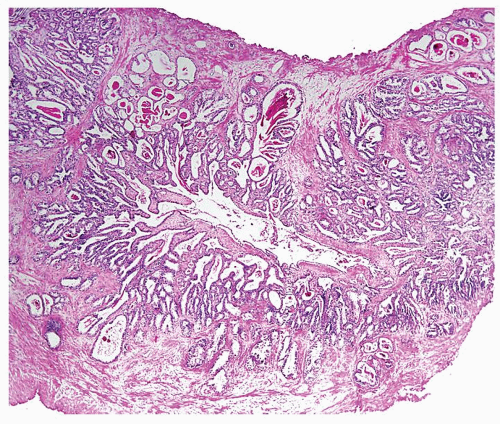 Figure 1.12.1 Seminal vesicle on a TURP showing central lumen surrounded by small glands. |
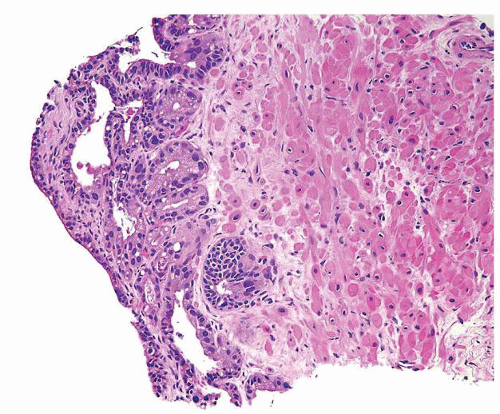 Figure 1.12.2 Needle biopsy with strip of seminal vesicle at edge (left) surrounded by small crowded glands. |
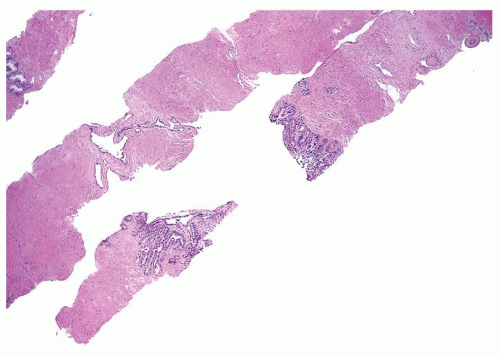 Figure 1.12.3 Needle biopsy with seminal vesicle epithelium on each side of break in tissue representing seminal vesicle lumen (bottom core). |
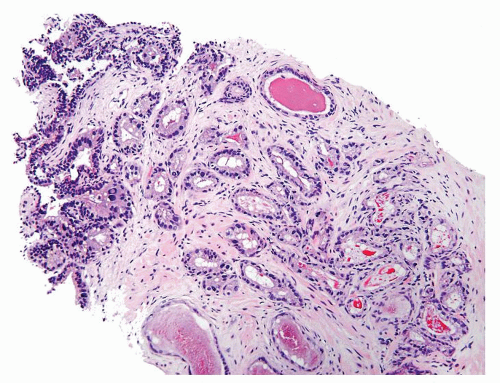 Figure 1.12.4 Needle biopsy with strip of seminal vesicle at edge (left) surrounded by small crowded glands. |
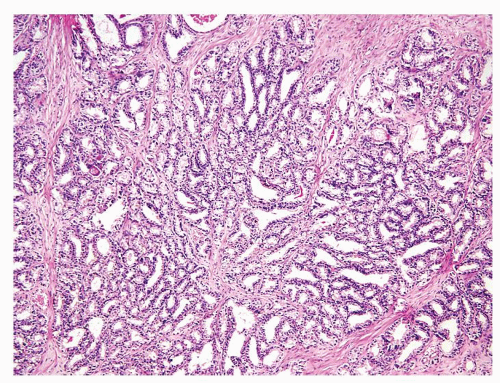 Figure 1.12.5 Crowded glands of seminal vesicle mimicking prostatic adenocarcinoma. |
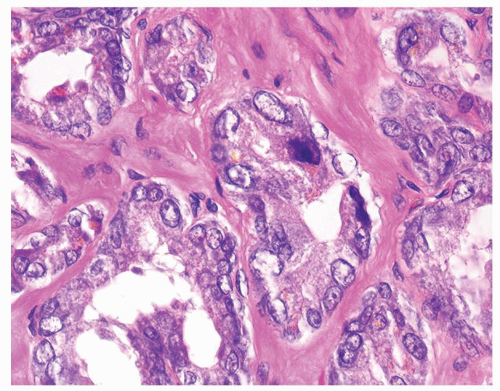 Figure 1.12.6 Higher magnification of Figure 1.12.5 where glands have degenerative atypia and golden brown lipofuscin pigment. |
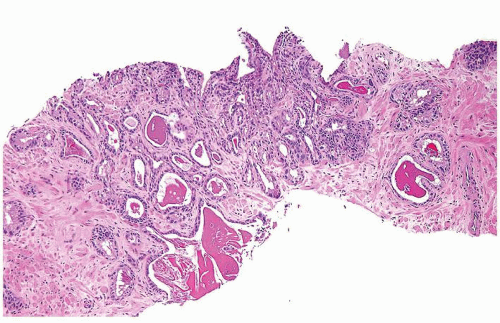 Figure 1.12.7 Crowded glands of seminal vesicle. |
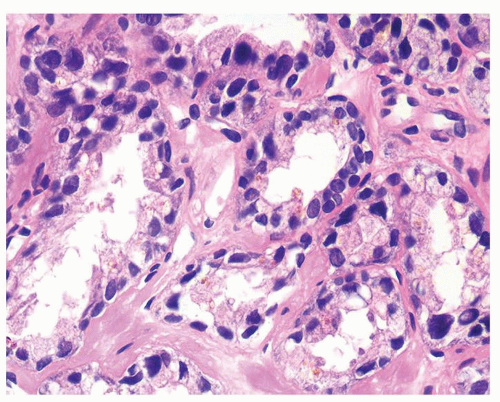 Figure 1.12.8 Same case as Figure 1.12.7 with glands showing degenerative atypia and golden brown lipofuscin pigment. |
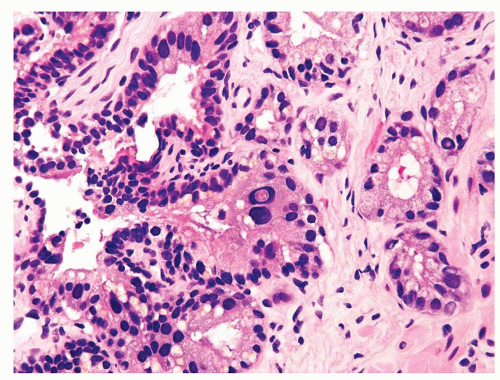 Figure 1.12.9 Degenerative atypia in seminal vesicle epithelium. |
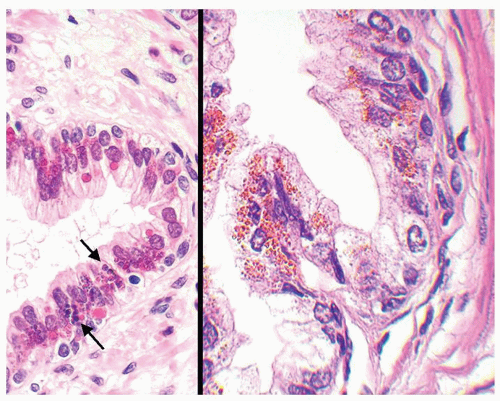 Figure 1.12.10 Benign prostate epithelium with small cytoplasmic blue (left, arrows) or red-orange (right) lipofuscin granules. |
|
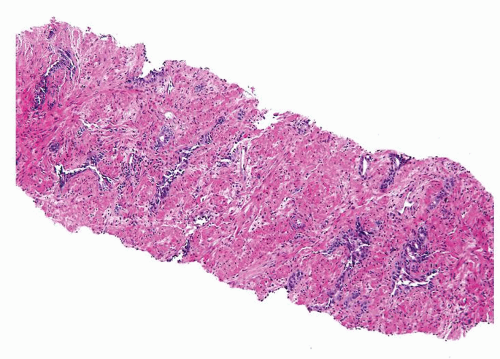 Figure 1.13.1 Benign prostate tissue with radiation atypia. At low magnification, glands are separated by a modest amount of stroma and are the size of normal benign prostate glands. Glands appear very blue due to atrophic cytoplasm. |
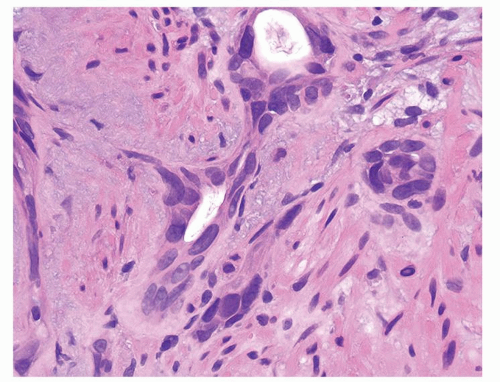 Figure 1.13.2 Atrophic benign-radiated glands. Scattered nuclei are enlarged and hyperchromatic. |
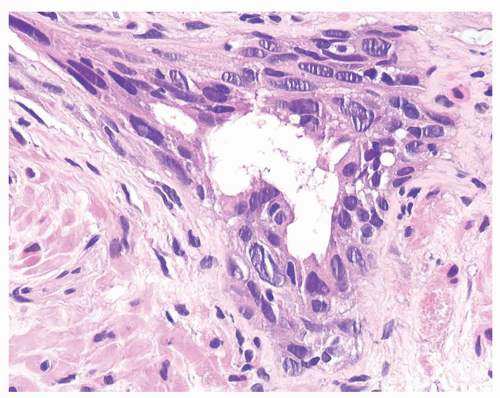 Figure 1.13.3 Multilayered benign-radiated gland with cells streaming parallel to the basement membrane. |
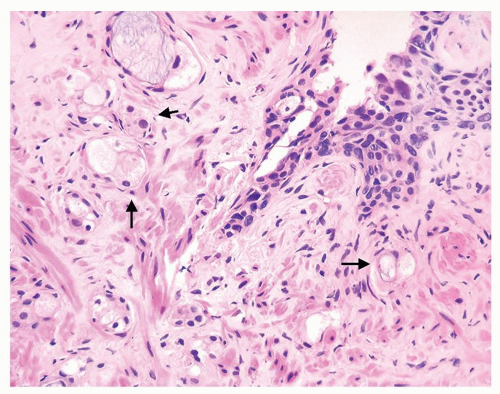 Figure 1.13.4 Scattered crowded smaller glands with vacuolated cytoplasm diagnostic of adenocarcinoma with treatment affect (arrows) adjacent to a larger multilayered benign gland with radiation atypia (upper right). |
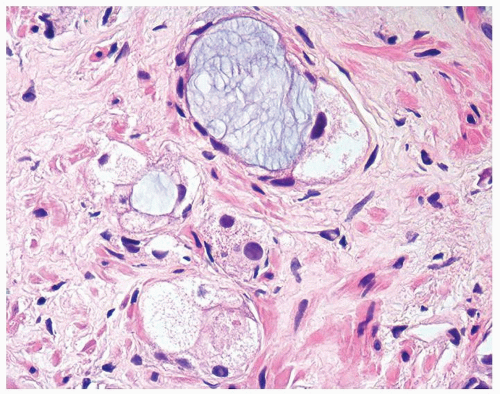 Figure 1.13.5 Higher magnification of Figure 1.13.4 with vacuolated crowded glands lined by bland nuclei. |
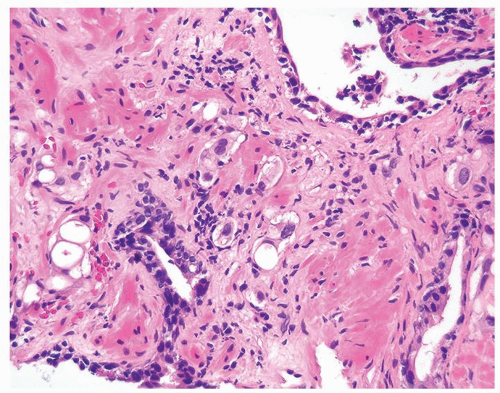 Figure 1.13.6 Radiated carcinoma with clusters of vacuolated cells invading between larger benign atrophic glands with radiation atypia. |
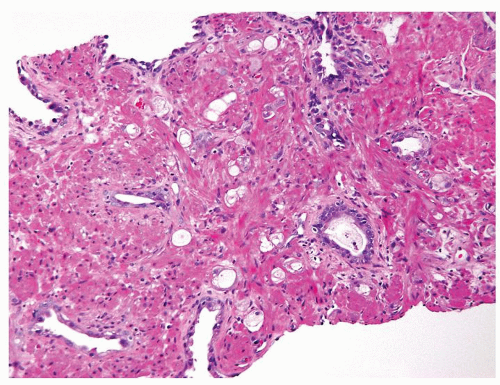 Figure 1.13.7 Crowded smaller glands with vacuolated cytoplasm diagnostic of adenocarcinoma with treatment affect in between darker, larger, more evenly spaced benign glands. |
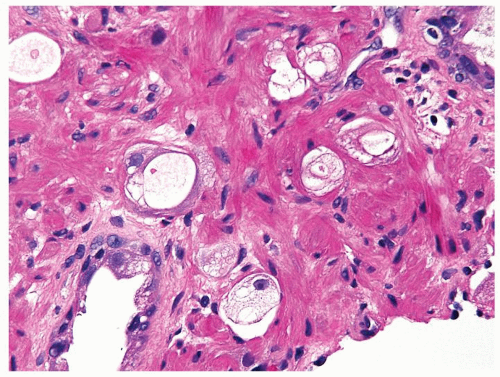 Figure 1.13.8 Higher magnification of Figure 1.13.7 with small vacuolated cancer glands (center) lacking prominent atypia invading between benign glands (lower left and upper right). |
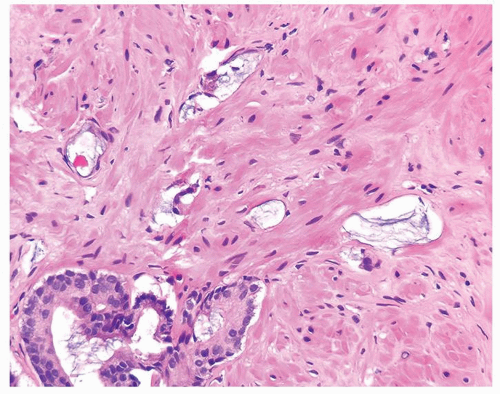 Figure 1.13.9 Atrophic glands of adenocarcinoma with abundant mucin showing treatment affect (top) adjacent to adenocarcinoma without treatment affect (lower left). |
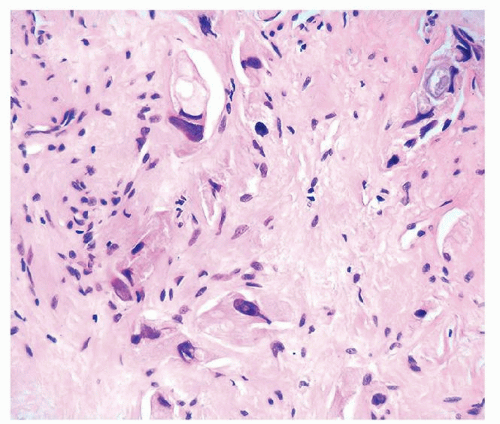 Figure 1.13.10 Adenocarcinoma with treatment affect with single cells with vacuolated cytoplasm. There is more prominent nuclear atypia, yet still with a degenerative appearance, than is typically seen in cancer with radiation affect. |
|
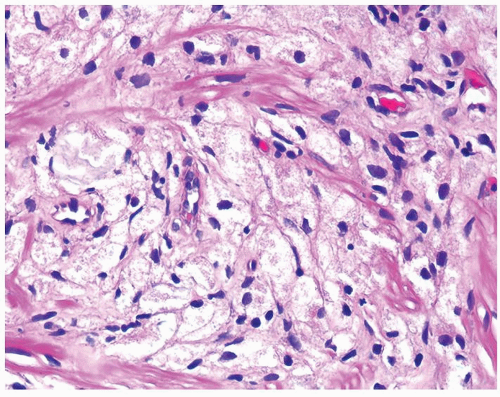 Figure 1.14.1 Xanthoma with bland cells. |
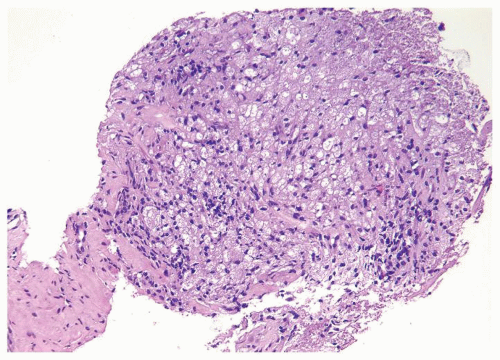 Figure 1.14.2 Cluster of xanthoma cells. |
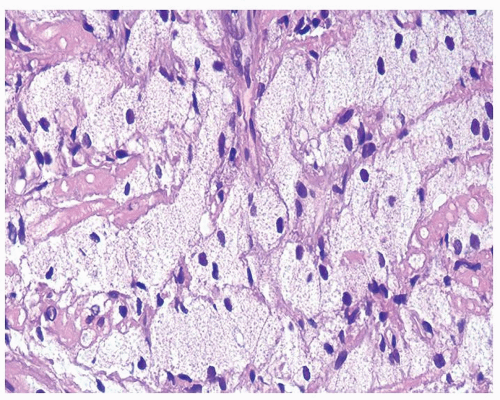 Figure 1.14.3 Bland cytology of xanthoma cells. |
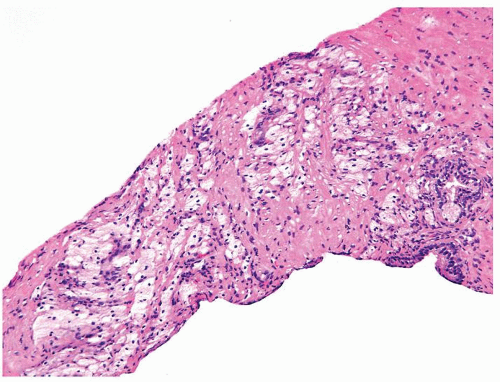 Figure 1.14.4 Cords of xanthoma cells. |
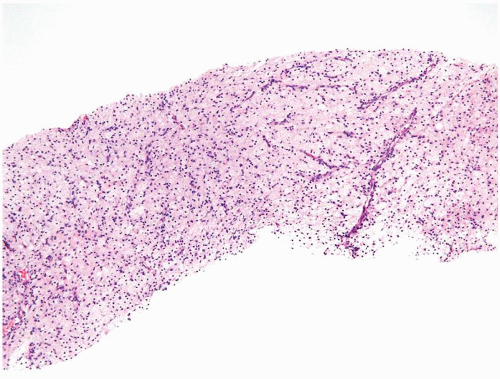 Figure 1.14.5 Unusual case of relatively extensive xanthoma on needle biopsy. |
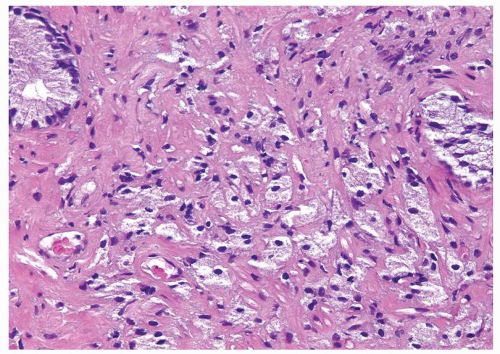 Figure 1.14.6 Individual cells and nests of xanthoma. |
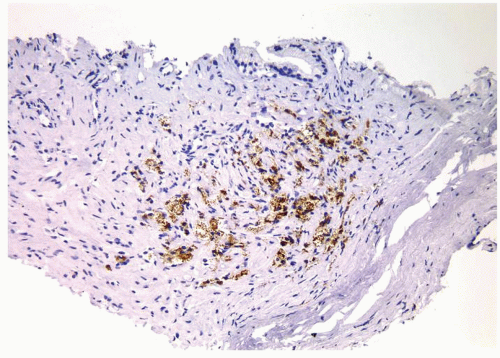 Figure 1.14.7 Same case as Figure 1.14.6 with positive staining for CD68. |
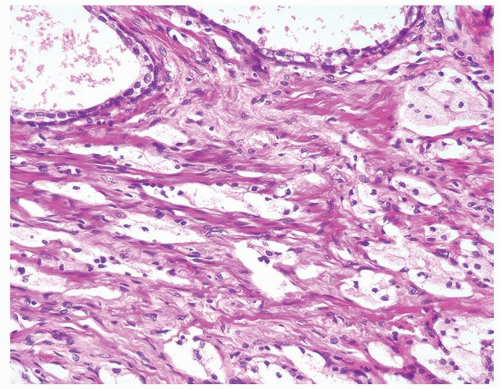 Figure 1.14.8 Adenocarcinoma with hormone treatment affect consisting of nests of cells with foamy cytoplasm in a slightly fibrotic stroma. |
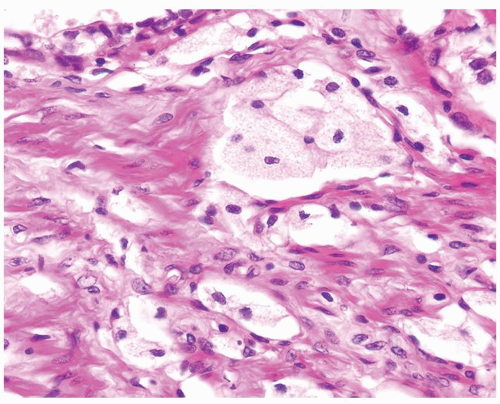 Figure 1.14.9 Higher magnification of Figure 1.14.8 showing cords of cells resembling xanthoma. Focal glandular differentiation is noted (top). |
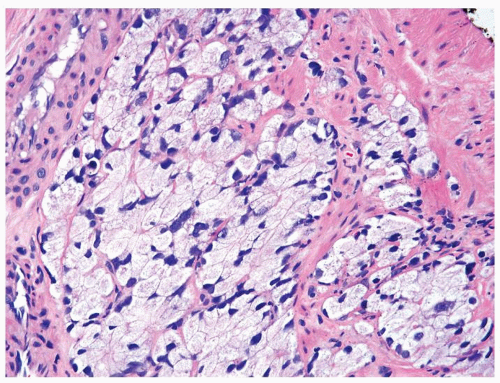 Figure 1.14.10 High-grade foamy gland adenocarcinoma. |
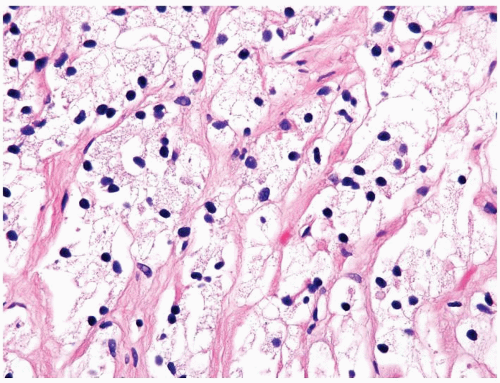 Figure 1.14.11 Hormone-treated prostate cancer with pyknotic hyperchromatic nuclei and abundant xanthomatous cytoplasm. |
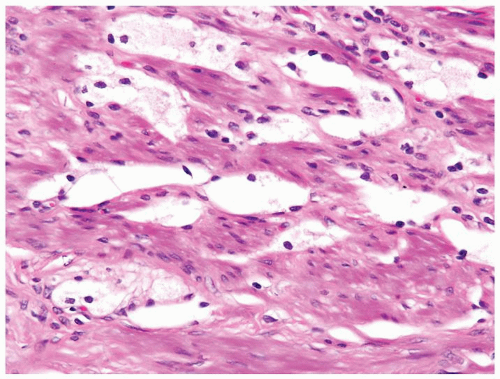 Figure 1.14.12 Adenocarcinoma of the prostate with hormone therapy affect with small nuclei, xanthomatous cytoplasm, and clear cleft-like spaces lined by pyknotic tumor nuclei resembling lymphocytes. |
|
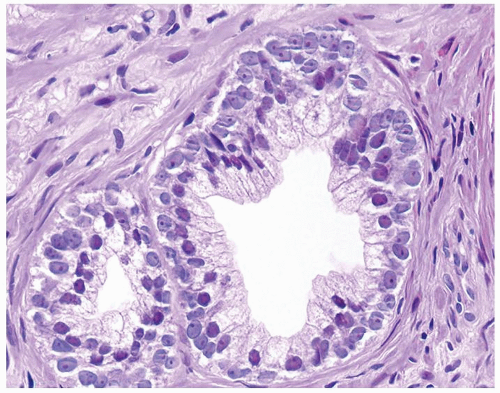 Figure 1.15.1 Basal cells with blue-gray nuclei containing prominent nucleoli undermine secretory cells with red-violet nuclei. |
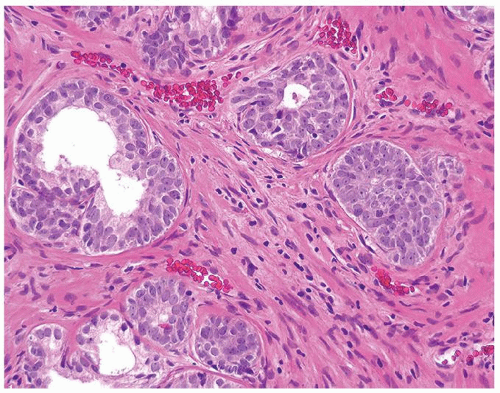 Figure 1.15.2 Proliferation of small glands of basal cell hyperplasia with prominent nucleoli. While one gland is larger resembling high-grade PIN (upper left), others are small with either a small central lumen with atrophic cytoplasm or composed of solid nests. |
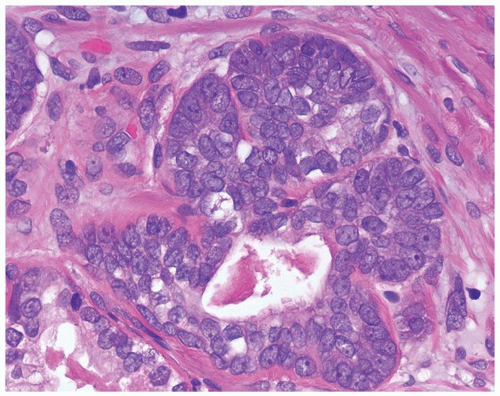 Figure 1.15.3 Basal cell hyperplasia with prominent nucleoli composed of solid nests surrounding the central lumen with atrophic cytoplasm. |
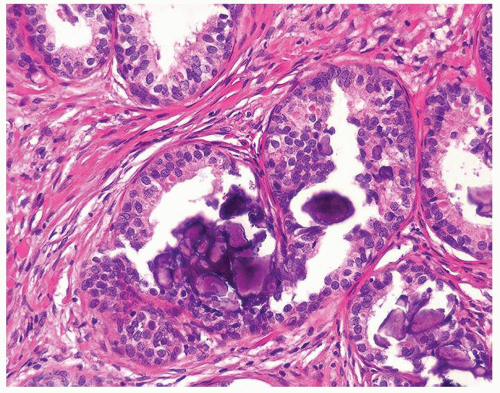 Figure 1.15.4 Basal cell hyperplasia with coarse calcifications. |
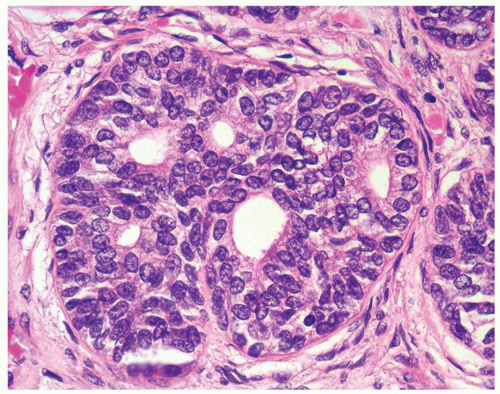 Figure 1.15.5 Pseudocribriform hyperplasia back-to-back glands of basal cell hyperplasia. |
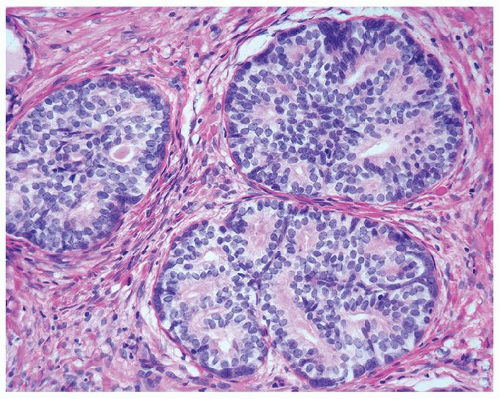 Figure 1.15.6 Pseudocribriform hyperplasia back-to-back glands of basal cell hyperplasia. Each gland maintains its integrity, where one can still identify each gland surrounding a lumen. |
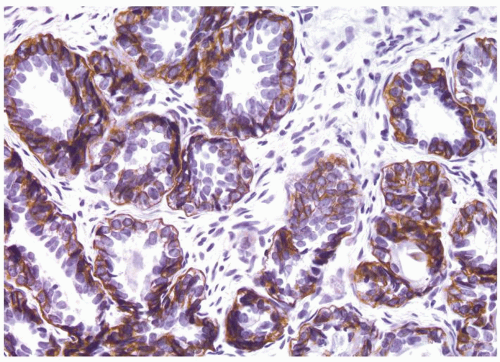 Figure 1.15.7 High molecular weight cytokeratin stain of basal cell hyperplasia labeling multilayered peripheral cells with prominent nucleoli. |
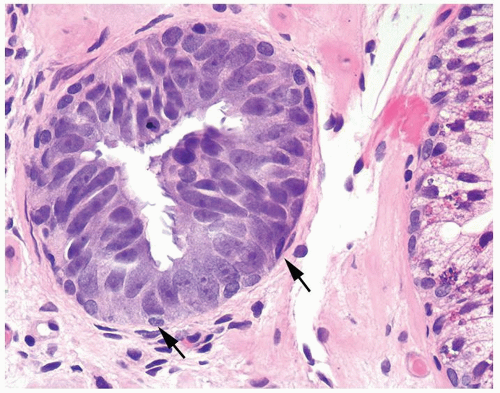 Figure 1.15.8 Tufted high-grade PIN with small basal cells (arrows) and overlying columnar PIN nuclei with prominent nucleoli. |
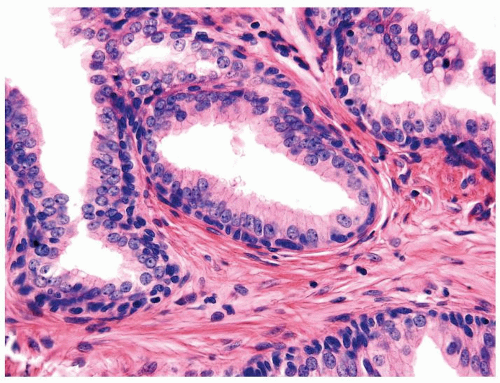 Figure 1.15.9 Flat high-grade PIN with small bland basal cells undermines columnar cells with nuclei containing prominent nucleoli. |
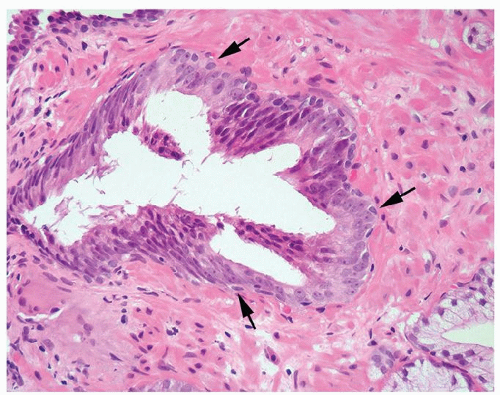 Figure 1.15.10 Tufted high-grade PIN with maturation of nuclei toward the center of the gland. However, note the presence of a distinct bland basal cell layer (arrows) with an abrupt transition to overlying atypical high-grade PIN nuclei. |
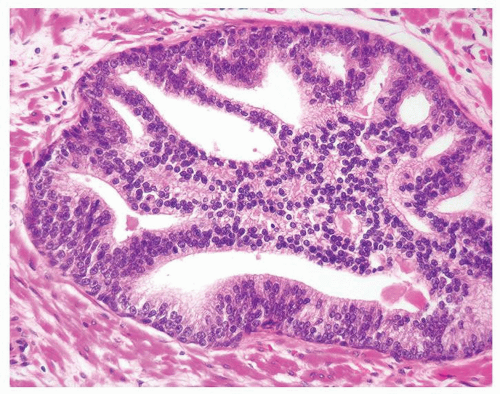 Figure 1.15.11 Cribriform high grade PIN. |
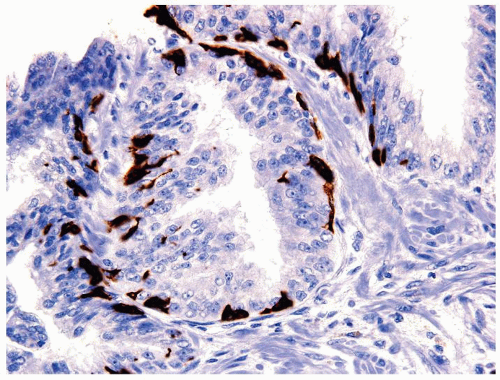 Figure 1.15.12 Patchy basal cell staining with p63 and high molecular weight cytokeratin. Overlying atypical PIN nuclei are negative. |
|
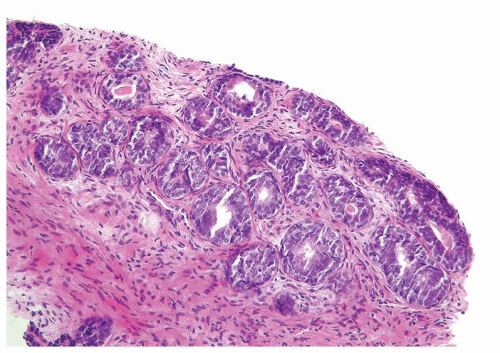 Figure 1.16.1 Basal cell hyperplasia on needle biopsy consisting of multilayered glands and solid nests. |
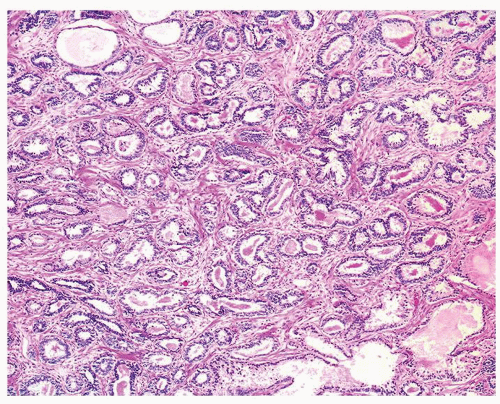 Figure 1.16.2 Basal cell hyperplasia. |
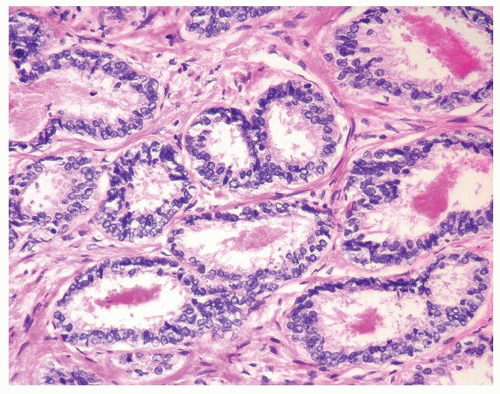 Figure 1.16.3 Same case as Figure 1.16.2 with two rows of basal cells and scant cytoplasm. |
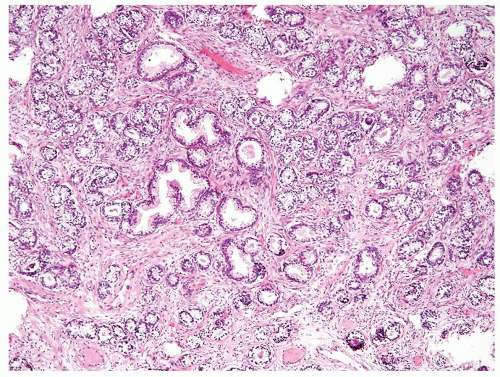 Figure 1.16.4 Basal cell hyperplasia glands interspersed between usual prostate glands. |
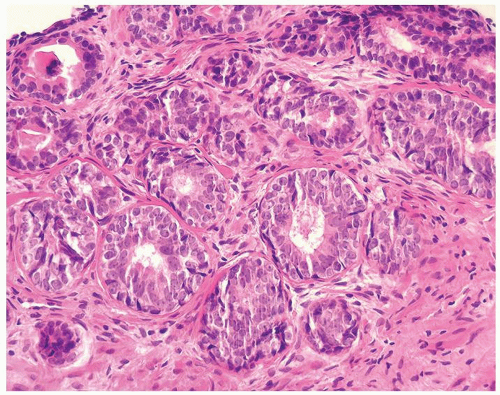 Figure 1.16.5 Basal cell hyperplasia with prominent nucleoli. |
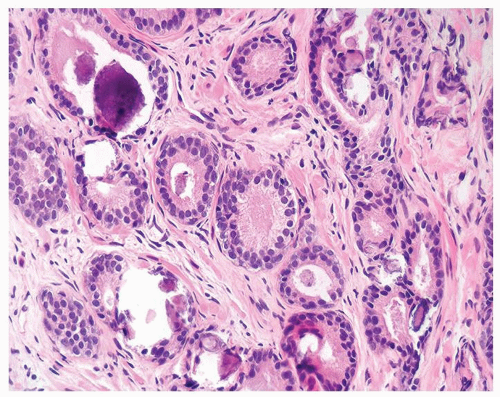 Figure 1.16.6 Basal cell hyperplasia with calcification. |
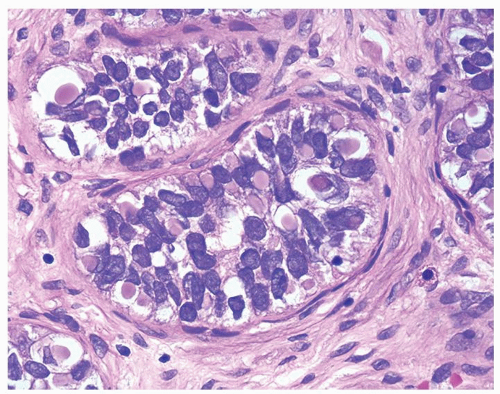 Figure 1.16.7 Same case as Figure 1.16.6 with numerous intracytoplasmic globules. |
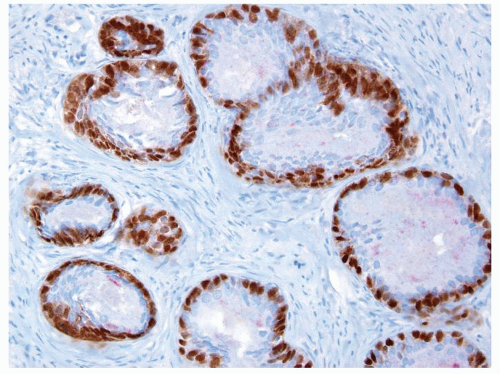 Figure 1.16.8 HMWCK and p63 staining of basal cell hyperplasia. |
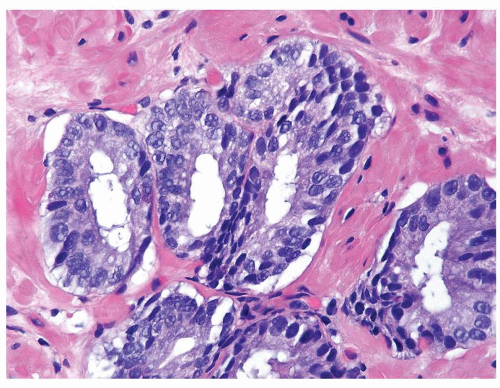 Figure 1.16.9 Adenocarcinoma with multilayered nuclei. |
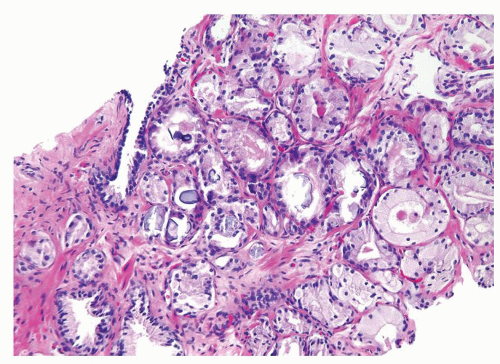 Figure 1.16.10 Adenocarcinoma with calcifications. |
|
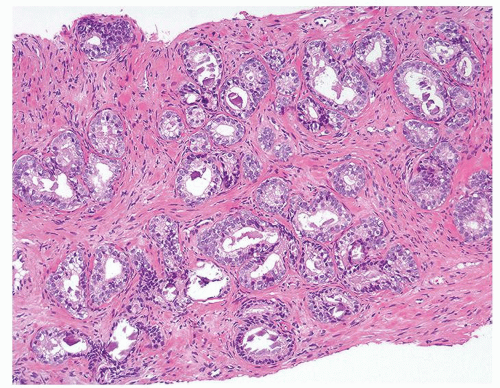 Figure 1.17.1 Basal cell hyperplasia on needle biopsy consisting of crowded, uniformly sized, and distributed small glands in prostatic stroma without a desmoplastic reaction. |
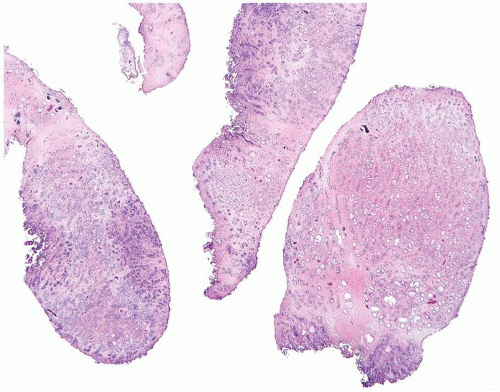 Figure 1.17.2 Extensive basal cell hyperplasia on TURP. |
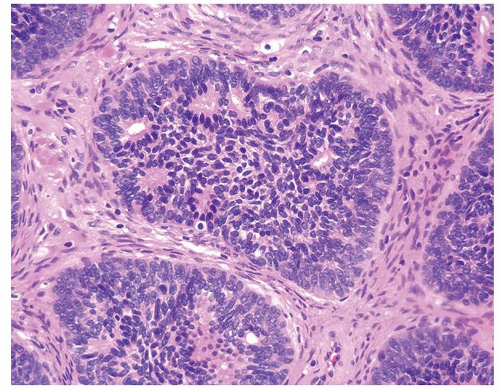 Figure 1.17.3 Pseudocribriform structure with individual well-defined glands surrounded by solid cells. |
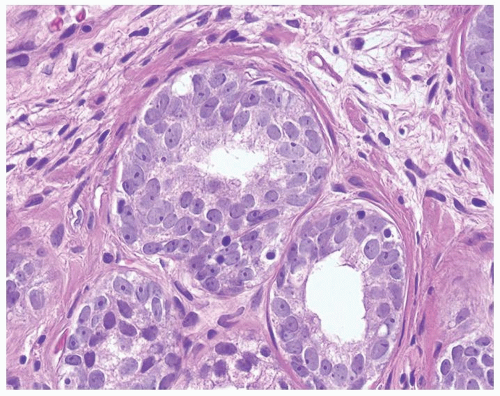 Figure 1.17.4 Basal cell hyperplasia with prominent nucleoli. |
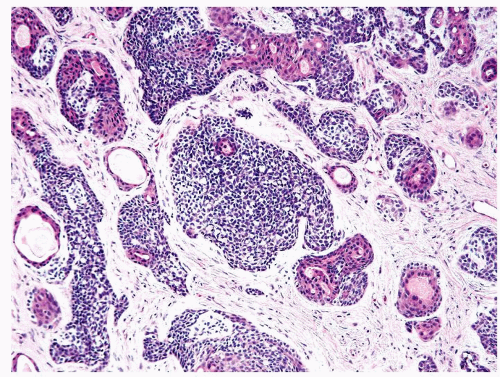 Figure 1.17.5 Basal cell carcinoma with irregular variably sized glands and nests in a desmoplastic stroma. Within inner aspect of some nests are tubules lined by eosinophilic cytoplasm. |
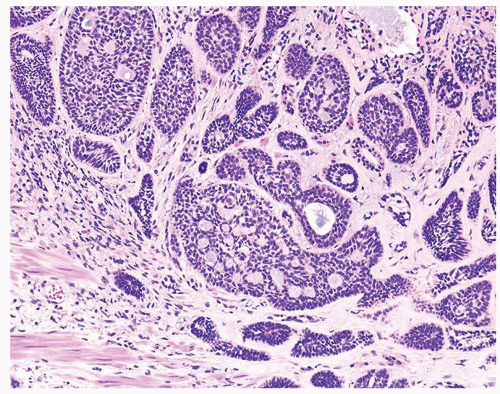 Figure 1.17.6 Small and medium nests of basal cell carcinoma in a desmoplastic stroma. |
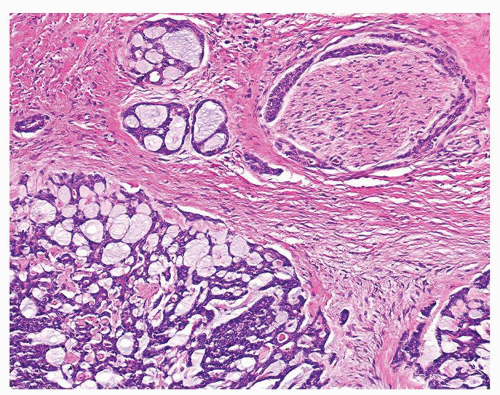 Figure 1.17.7 Adenoid cystic pattern of basal cell carcinoma with perineural invasion. |
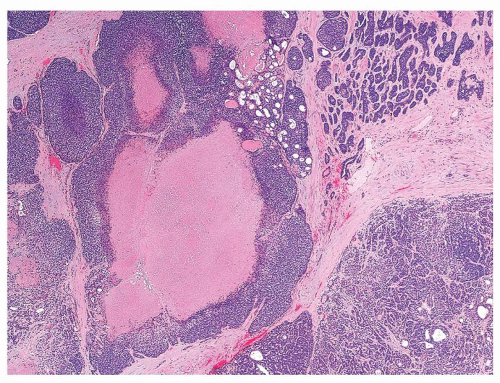 Figure 1.17.8 Basal cell carcinoma with solid nests with necrosis. |
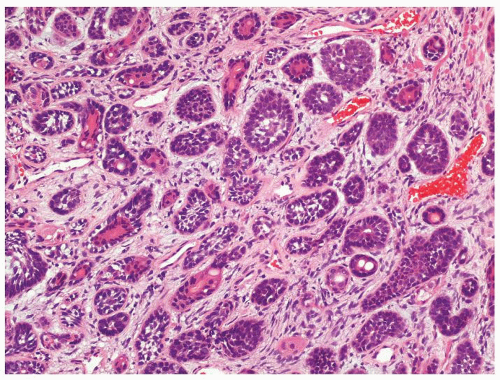 Figure 1.17.9 Small nests of basal cell carcinoma with tubules lined by eosinophilic cytoplasm. |
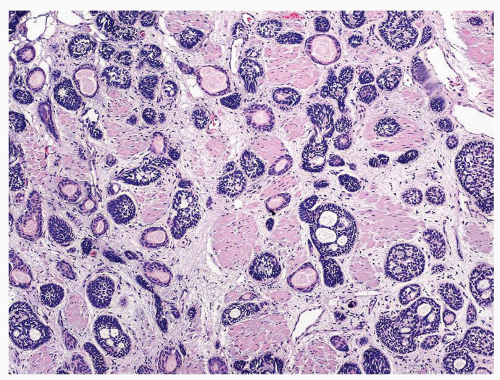 Figure 1.17.10 Basal cell carcinoma resembling basal cell hyperplasia. Nests and tubules infiltrated thick bladder neck muscle diagnostic of carcinoma. |
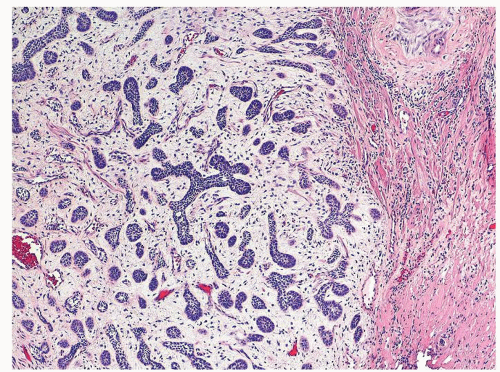 Figure 1.17.11 Basal cell carcinoma with prominent myxoid stromal reaction. |
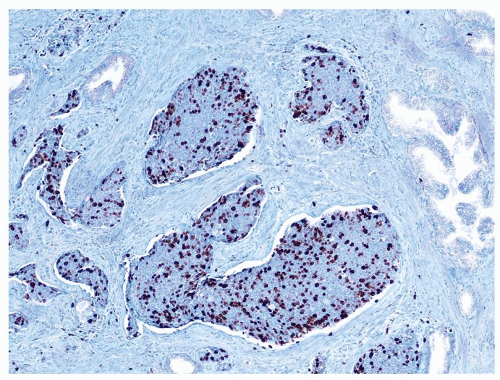 Figure 1.17.12 Elevated Ki-67 in basal cell carcinoma. |
|
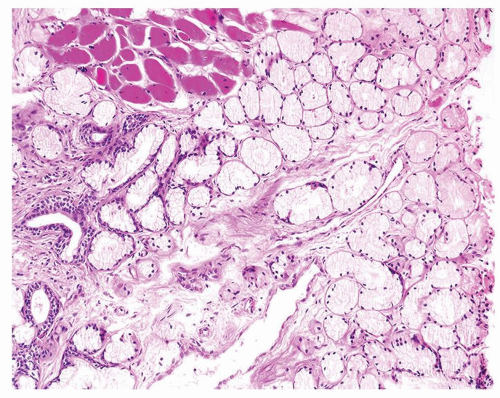 Figure 1.18.1 Cowper glands in skeletal muscle. |
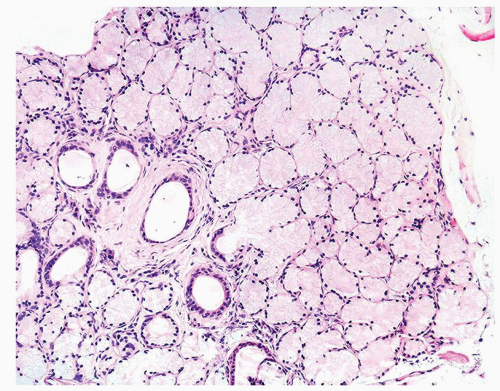 Figure 1.18.2 Lobular Cowper glands with mucinous glands and atrophic ducts lined by cuboidal nonmucinous epithelium. Distended cytoplasm results in small central lumina. |
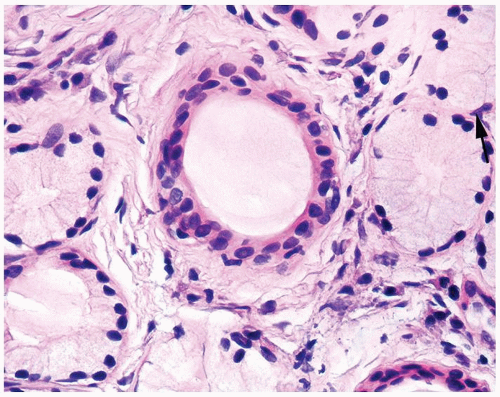 Figure 1.18.3 Higher magnification of Figure 1.18.2 with central duct and surrounding mucinous glands. Some cells have rounded distended appearance (arrow). |
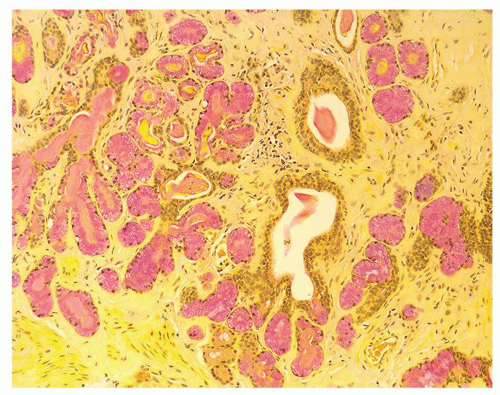 Figure 1.18.4 Mucicarmine-positive Cowper glands. |
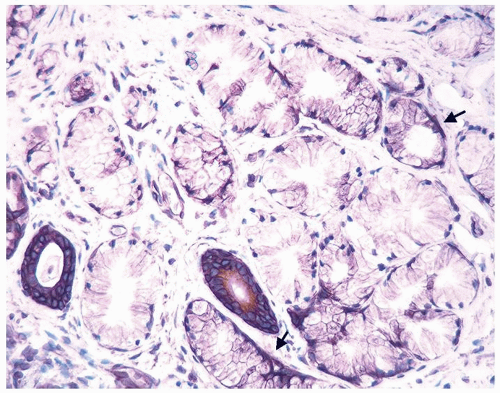 Figure 1.18.5 Cowper glands lined by HMWCK-positive basal cells (arrows). |
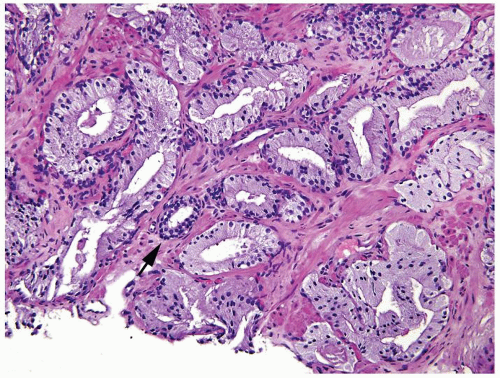 Figure 1.18.6 Foamy gland carcinoma infiltrating in prostate stroma around the benign gland (arrow). |
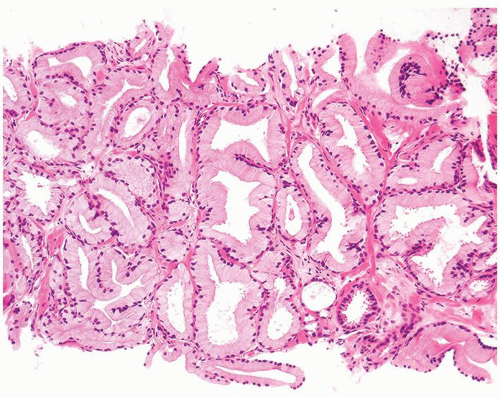 Figure 1.18.7 Foamy gland carcinoma with crowded glands with well-formed open lumina. |
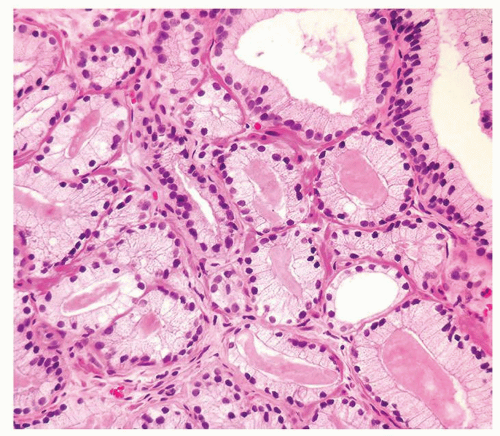 Figure 1.18.8 Dense pink secretions in a foamy gland carcinoma. |
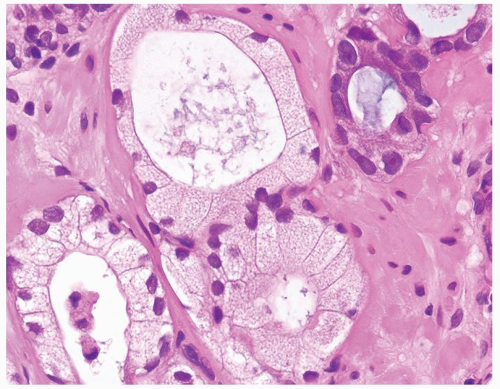 Figure 1.18.9 Foamy gland carcinoma with cuboidal to columnar bland nuclei. More atypical nuclei are seen in adjacent nonfoamy gland carcinoma (upper right). |
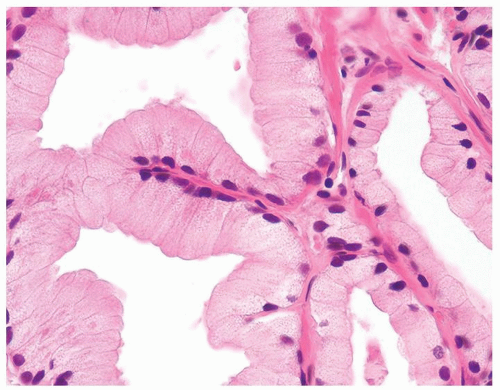 Figure 1.18.10 Foamy gland carcinoma with bland nuclei and columnar cells with abundant xanthomatous-appearing cytoplasm. |
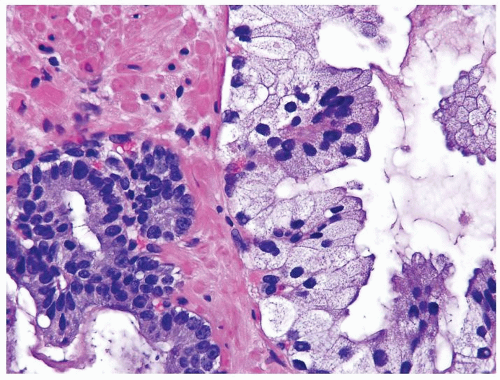 Figure 1.18.11 Foamy gland carcinoma (right) with bland nuclei compared to usual prostate cancer with greater cytologic atypia (left). |
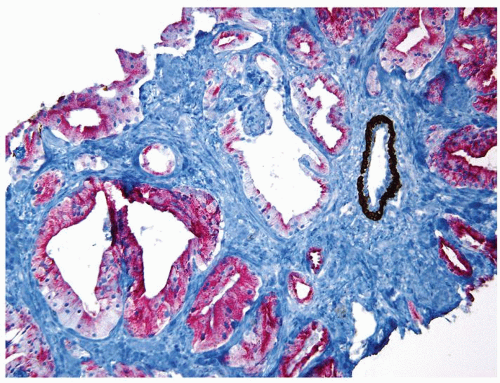 Figure 1.18.12 Foamy gland carcinoma lacking basal cells (brown) and positive for AMACR (red). An entrapped benign gland surrounded by basal cells is present (same case as Fig. 1.18.6). |
|
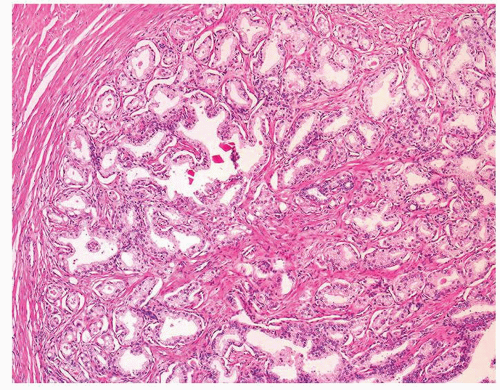 Figure 1.19.1 Lobular focus of adenosis. Glands lack interspersed large bundles of smooth muscle. |
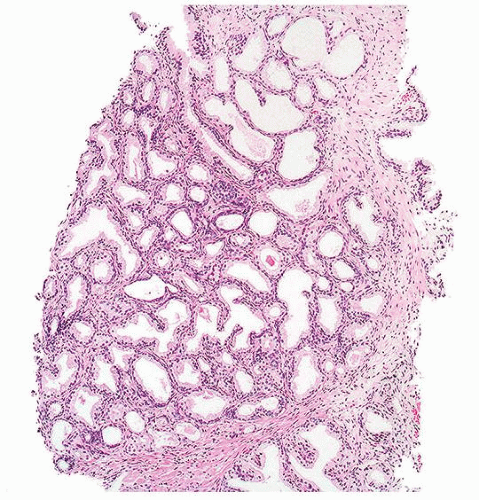 Figure 1.19.2 Adenosis on needle where a lobular pattern can still be appreciated. |
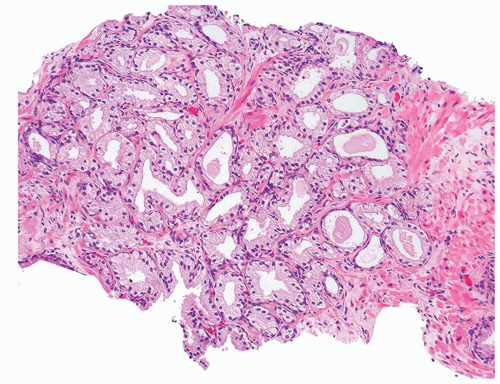 Figure 1.19.3 Adenosis on needle biopsy. |
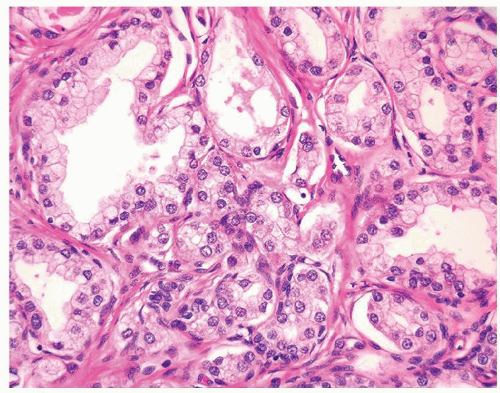 Figure 1.19.4 Same case as Figure 1.19.1 with small crowded glands sharing cytoplasmic and nuclear features with more benign-appearing glands (left). |
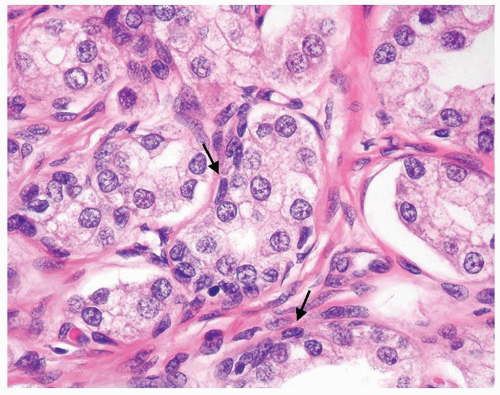 Figure 1.19.5 Same case as Figure 1.19.1 with some glands with a visible basal cell layer (arrows). Some of the glands are tangentially sectioned (left). |
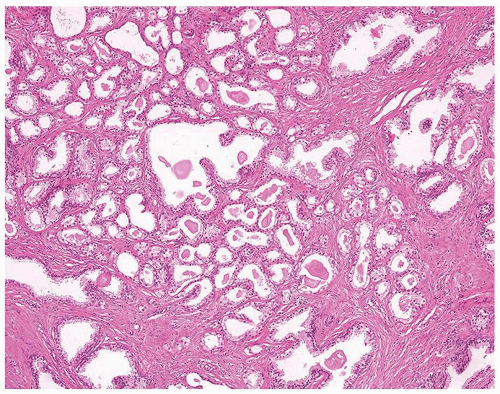 Figure 1.19.6 Adenosis with corpora amylacea. |
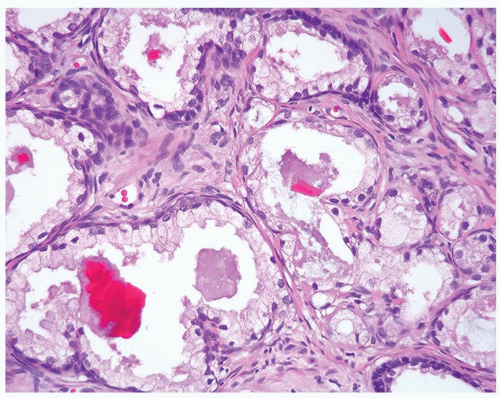 Figure 1.19.7 Same case as Figure 1.19.1 with crystalloids. |
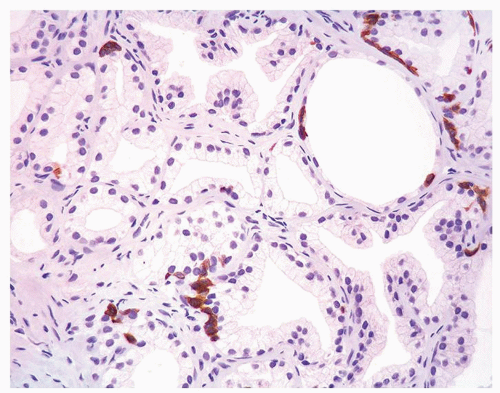 Figure 1.19.8 Same case as Figure 1.19.1 with adenosis showing some glands with HMWCK patchy, positive basal cells and other glands negative. Negative glands have the same morphology as positive glands. |
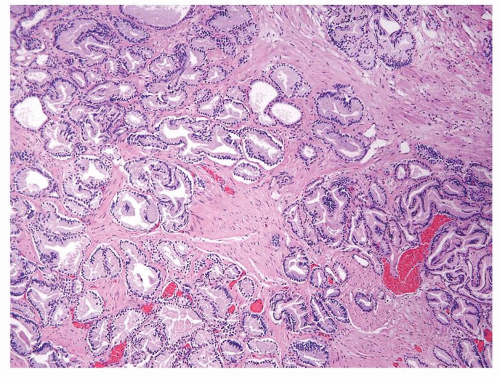 Figure 1.19.9 Irregular growth pattern of cancer with glands interspersed between large bundles of smooth muscle. |
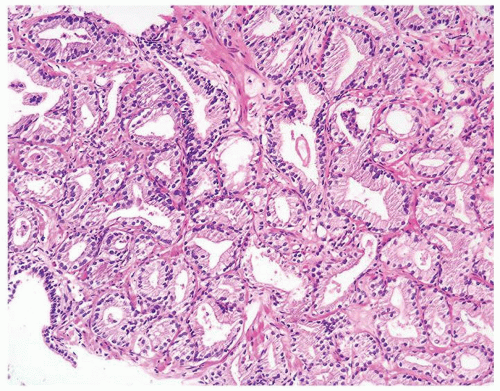 Figure 1.19.10 Adenocarcinoma mimicking adenosis on needle biopsy. |
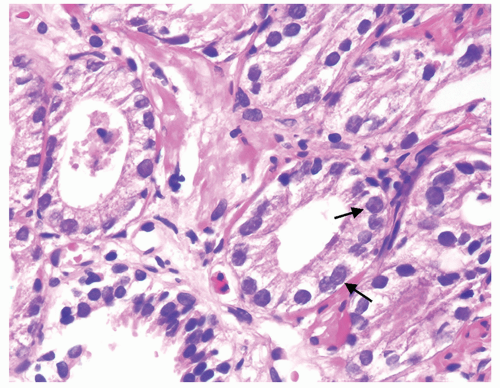 Figure 1.19.11 Same case as Figure 1.19.10 with adenocarcinoma showing prominent nucleoli (arrows) compared to benign gland (lower left). |
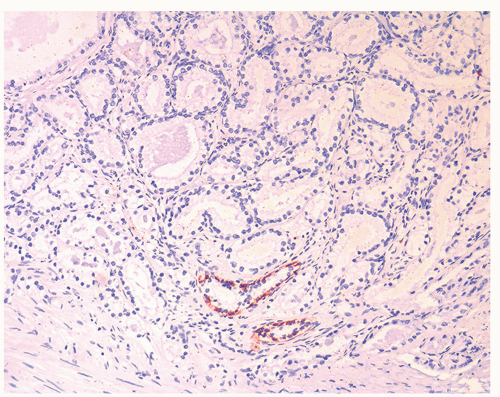 Figure 1.19.12 Negative stains for HMWCK (same case as Figs. 1.19.10 and 1.19.11). Note entrapped benign glands (bottom) with circumferential staining. |
|
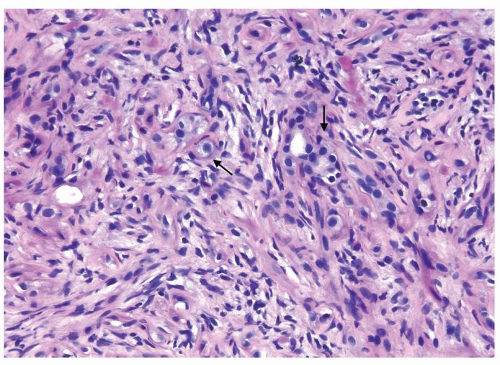 Figure 1.20.1 Sclerosing adenosis with scattered glands and single epithelial cells (arrows) with cellular stroma background. |
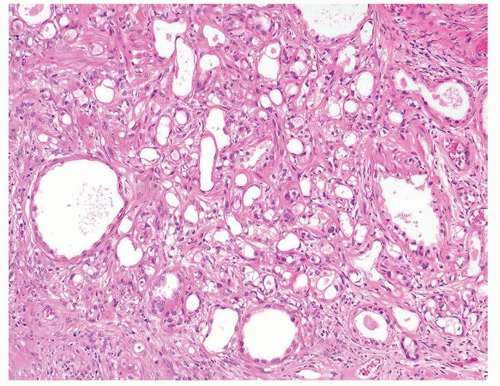 Figure 1.20.2 Limited focus of sclerosing adenosis on TURP. |
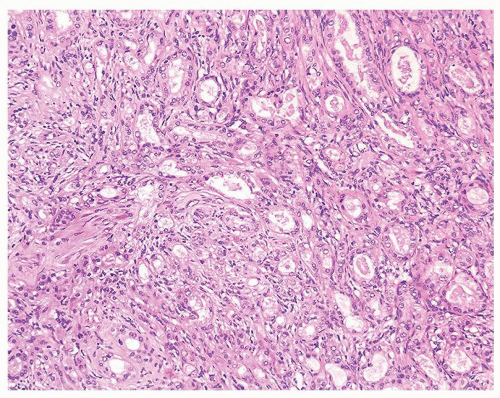 Figure 1.20.3 Sclerosing adenosis consisting of well-formed glands (right) and poorly formed glands (left) with cellular spindle cells in background. |
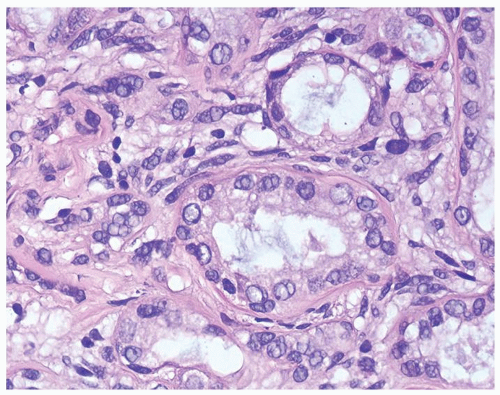 Figure 1.20.4 Higher magnification of Figure 1.20.2 showing a gland surrounded by hyaline rim of connective tissue. Background of cellular spindle cells. |
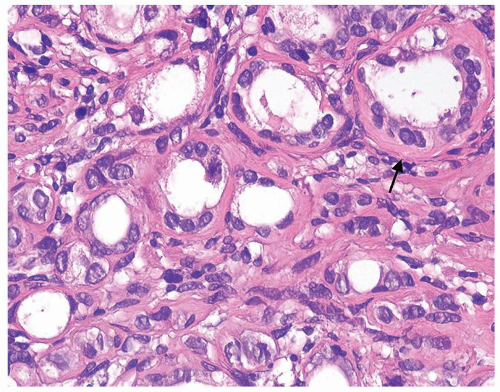 Figure 1.20.5 Higher magnification of Figure 1.20.3 with atrophic glands having hyaline rim (arrow). |
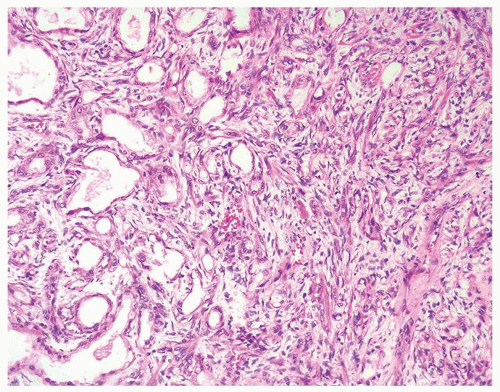 Figure 1.20.6 Sclerosing adenosis. |
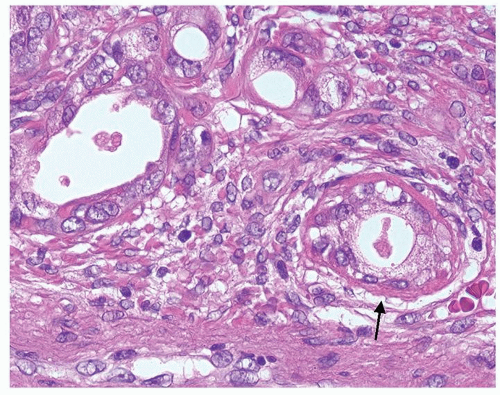 Figure 1.20.7 Higher magnification of Figure 1.20.6 with a gland having hyaline rim of connective tissue (arrow). Glands have nuclei with prominent nucleoli. |
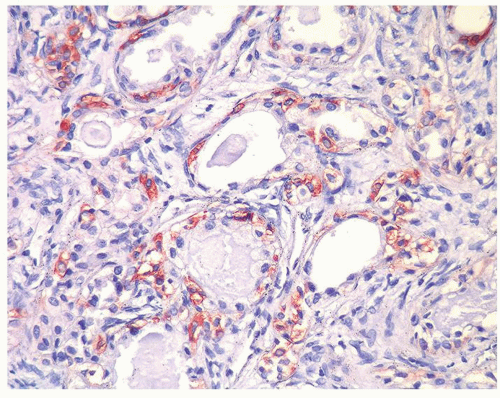 |
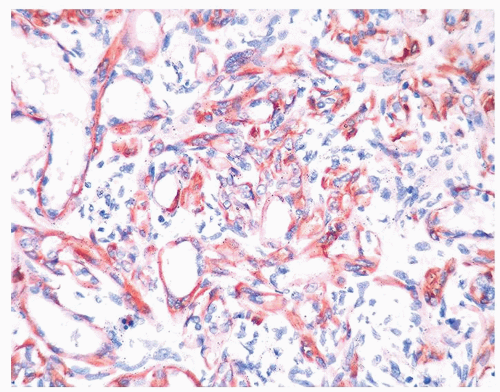 Figure 1.20.9 Same case as Figures 1.20.6, 1.20.7, 1.20.8 with S100 protein showing myoepithelial cell differentiation in basal and some spindle cells. |
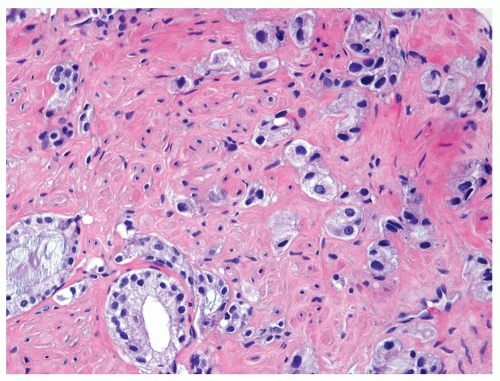 Figure 1.20.10 Adenocarcinoma, Gleason score 5 + 3 = 8 lacking cellular background stroma and hyaline rim of connective tissue around glands. |
|
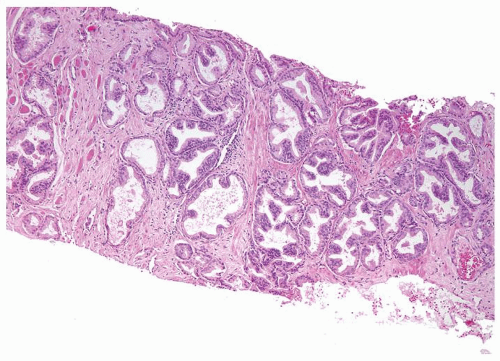 Figure 1.21.1 Pseudohyperplastic carcinoma with large crowded glands with papillary infolding. |
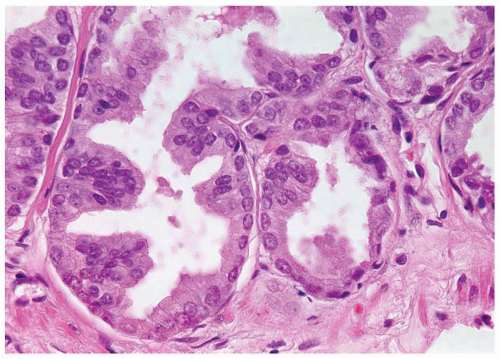 Figure 1.21.2 Same case as Figure 1.21.1 with numerous prominent nucleoli. |
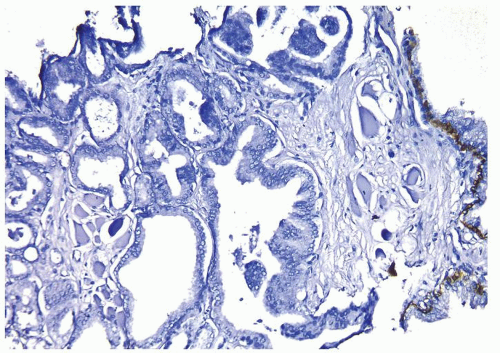 Figure 1.21.3 Same case as Figures 1.21.1 and 1.21.2 with absence of a basal cell layer. Note benign gland with basal cells (right). |
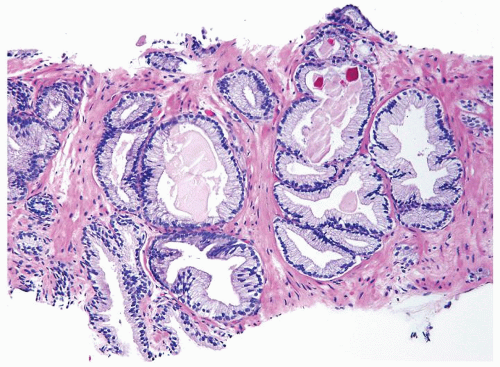 Figure 1.21.4 Pseudohyperplastic carcinoma with crowded glands with papillary infolding. |
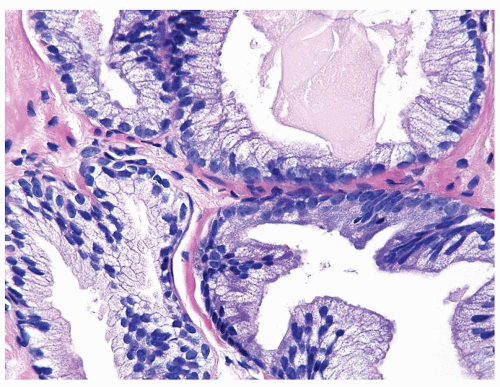 Figure 1.21.5 Same case as Figure 1.21.4 with numerous prominent nucleoli in cancer glands (right) compared to benign gland (lower left). Stains showed an absence of basal cells. |
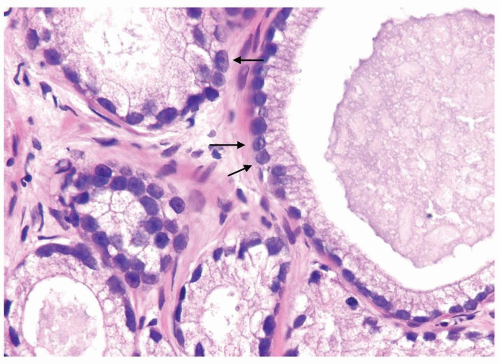 Figure 1.21.6 Pseudohyperplastic carcinoma with large glands with straight luminal borders and abundant cytoplasm and prominent nucleoli (arrows). |
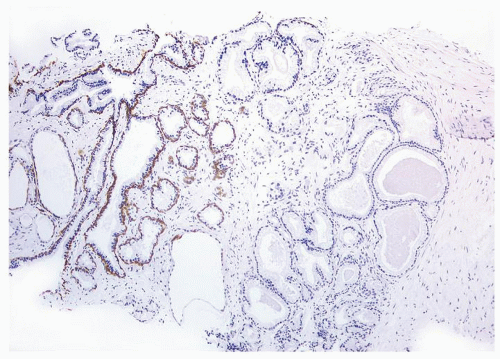 Figure 1.21.7 Same case as Figure 1.21.6 with absence of a basal cell layer in large glands with straight luminal border (right). Less crowded benign glands without atypia have a basal cell layer (left). |
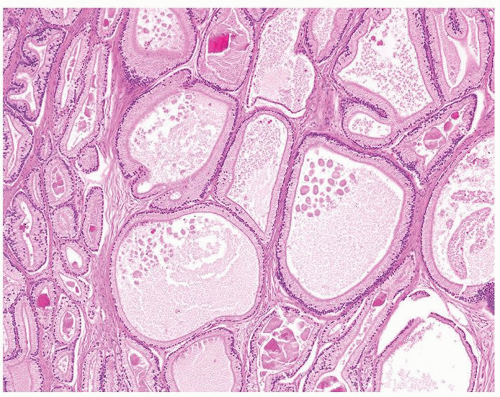 Figure 1.21.8 Pseudohyperplastic carcinoma with large glands with straight luminal borders and abundant cytoplasm. |
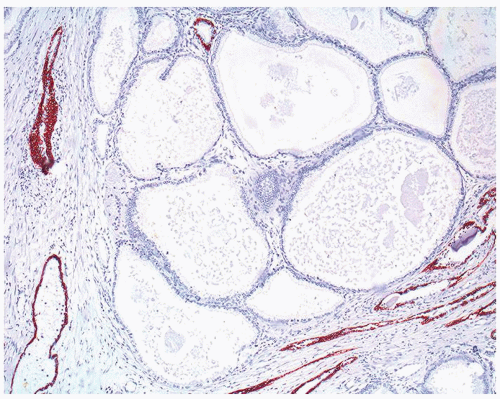 Figure 1.21.9 Same case as Figure 1.21.8 with absence of a basal cell layer in large glands with straight luminal border. |
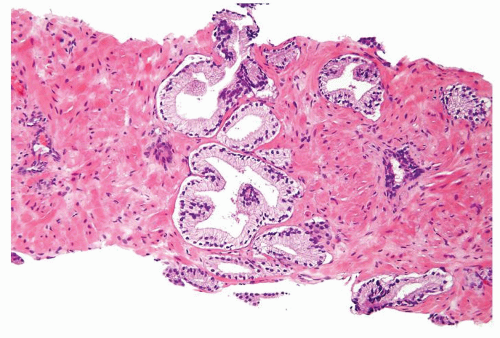 Figure 1.21.10 Benign crowded cluster of larger glands with papillary infolding. |
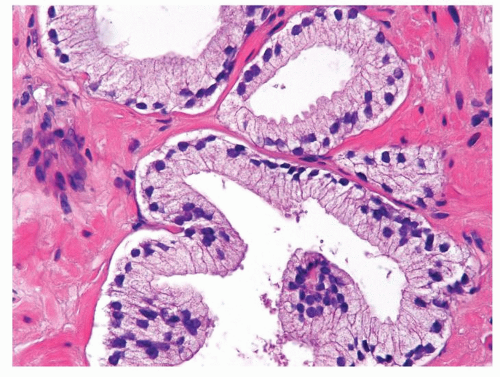 Figure 1.21.11 Same case as Figure 1.21.10 with totally benign cytology. |
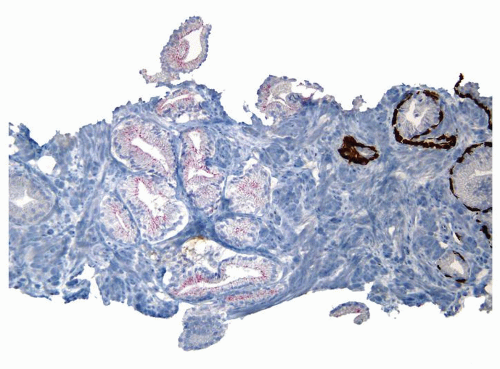 Figure 1.21.12 Same case as Figures 1.21.10 and 1.21.11 with absence of a basal cell layer. As the focus on H&E is totally benign, negative staining for basal cells in a small focus of glands is still consistent with a benign diagnosis. |
|
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


