Prenatal Case Study
Dale Halsey Lea MPH, RN, CGC, APNG, FAAN
Background
Apediatric neurologist referred a couple, Mr. and Mrs. R., whose two year-old identical twin girls had recently been diagnosed with the rare neurodegenerative condition metachromatic leukodystropy (MLD), to our Medical Center Division of Genetics. The couple sought more information about “how this had happened to them,” and what the chances were that they would have more children with the same condition. The twins, at the time of referral, had developed seizures and had lost their ability to walk.
Patient and Family Profile
Pregnancy History: Mrs. R.’s pregnancy with her twin girls was uncomplicated. She delivered them at 38 weeks via cesarean section. Both girls were assessed as healthy at birth. They were in the newborn nursery for three days before being discharged home.
Developmental History: Both girls developed normally until they were 15 months. Both began to develop gait disturbances and loss of fine motor abilities such as feeding themselves. One of the girls had a seizure at 16 months. They were referred to the pediatric neurologist at that point.
Diagnosis: Evaluation of the twins included a physical examination, which revealed that they both had developmental deterioration and diminished deep tendon reflexes. The following diagnostic studies were conducted for further evaluation:
Brain MRI (magnetic resonance imaging): Both were abnormal, with white matter lesions and atrophy, characteristic of MLD.
Leukocyte (white blood cells) cultures for arylsulfatase A enzyme activity— severely depressed activity of arylsulfatase A in leukocytes in both girls. This is generally considered diagnostic, leaving little doubt about the nature of the condition.
Based on these results, a diagnosis of MLD was made. The neurologist explained to Mr. and Mrs. R. that MLD is rare (1 in 40,000 individuals), and that there are several types. The type present in their daughters is the late infantile form in which symptoms appear at 4 years or younger. Typically, these children experience gait disturbances, loss of motor developmental milestones (normally expected neuromuscular function), optic atrophy, and diminished deep tendon reflexes. Progressive loss of both motor and cognitive functions is usually rapid and the children die usually within 5 years after the onset of clinical symptoms.
At the time of their diagnosis (2000), there was no effective treatment available to reverse the deterioration and loss of function. Bone marrow transplantation was available to stabilize neurocognitive function, but symptoms of motor function loss frequently progress even with this intervention. Gene therapy was under development as a possible solution, but at that time was still under investigation and not ready for clinical trials (Moore 2006; United Leukodystrophy Foundation 2008). Supportive care could be provided as needed for feeding difficulties, seizure disorder, and constipation.
Family History: A three-generation family history was taken on both Mrs. R. and Mr. R. (see pedigree in Figure 23-1). In the review of family history, Mr. and Mrs. R. noted the following issues of significance:
Mrs. R. is one of three siblings. All are in good health. Her younger brother had a son who was born with a congenital heart defect (ventriculoseptal defect, VSD). He is in good health.
Mrs. R.’s mother has a history of heart disease. She is 62 years old.
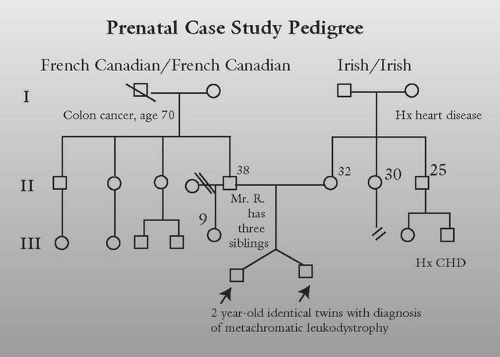
FIGURE 23-1 R Family Pedigree
Mr. R. is one of three siblings. All are in good health as are their children.
Mr. R. has a nine-year-old daughter from a previous relationship. She is in good health.
Mr. R.’s father died from complications related to colon cancer at the age of 71.
Mrs. R. is of Irish ancestry and Mr. R. is of French Canadian ancestry. There is no history of consanguinity (biological relatedness).
Objective
Mr. and Mrs. R. came for their genetic counseling appointment and brought their twin girls with them. At the time that we provided genetic counseling, the girls had lost any speech that they had. They had recently undergone an ophthalmology evaluation that showed the beginnings of optic atrophy in both girls. Mr. and Mrs. R. explained that they were “still reeling from the diagnosis three months ago.” Mrs.
R. stated, “I had such a healthy pregnancy, and our families are so healthy, I just can’t believe that this is happening to us.” The couple had many questions about the cause of MLD and the chance for having another child with MLD. Mr. R. said “We so want to have more children, especially since our girls will not be with us for very long. But is it possible to have a healthy child together?” At this time, the focus of the couple’s concern was on the cause of MLD and recurrence. Therefore, the focus of the consultation was on explaining the inheritance of MLD, recurrence in future children and available prenatal testing. A physical examination of the girls was not indicated.
R. stated, “I had such a healthy pregnancy, and our families are so healthy, I just can’t believe that this is happening to us.” The couple had many questions about the cause of MLD and the chance for having another child with MLD. Mr. R. said “We so want to have more children, especially since our girls will not be with us for very long. But is it possible to have a healthy child together?” At this time, the focus of the couple’s concern was on the cause of MLD and recurrence. Therefore, the focus of the consultation was on explaining the inheritance of MLD, recurrence in future children and available prenatal testing. A physical examination of the girls was not indicated.
Family and Social Profile
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


