Porokeratosis
George R. Collins, DO
Joseph Susa, DO
Clay J. Cockerell, MD
Key Facts
Terminology
Porokeratosis: Genodermatosis with clonal keratinocytes resulting in clinically and morphologically distinct keratinization disorder
Several clinical variants of porokeratosis with overlapping features exist among described varieties
Clinical Issues
Porokeratosis of Mibelli manifests as 1 or more asymptomatic large, round to oval, skin-colored to red to brown, annular plaques often occurring unilaterally on extremities
DSAP has many superficial, coalescent, small, thin, keratotic, skin-colored to red to brown annular plaques or papules with peripheral cornoid lamella occurring bilaterally on sun-exposed extremities
Porokeratosis has prolonged course, is hard to treat
Microscopic Pathology
Cornoid lamella is the hallmark feature of all variants and corresponds to clinically evident raised hyperkeratotic peripheral ridge of lesion
Cornoid lamella is a thin, compact column of parakeratosis; granular layer is absent to decreased, and dyskeratotic keratinocytes are present at the base
Top Differential Diagnoses
Cornoid lamella are not specific for porokeratosis and can be seen in neoplastic (actinic keratosis, carcinomas) or reactive (viral warts) squamous proliferations as well as in normal skin
Benign lichenoid keratosis and clinically linear lesions are also in differential diagnosis
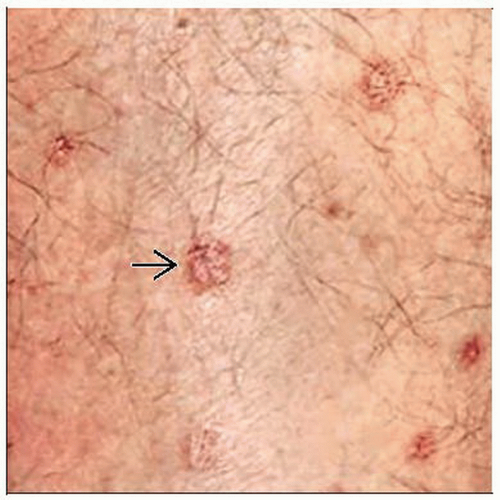 Disseminated superficial actinic porokeratosis presents here as multiple, small, well-demarcated, erythematous, annular plaques  with raised hyperkeratotic peripheral ridges (cornoid lamellae). with raised hyperkeratotic peripheral ridges (cornoid lamellae). |
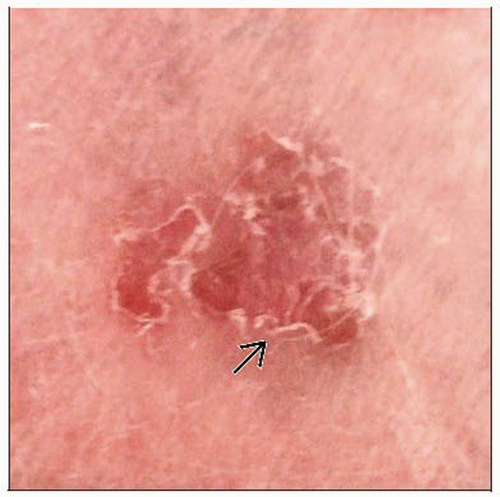 Porokeratosis of Mibelli demonstrates a sharply demarcated oval plaque with an erythematous center surrounded by a raised, hyperkeratotic, peripheral ridge that represents the cornoid lamella  . . |
TERMINOLOGY
Abbreviations
Disseminated superficial actinic porokeratosis (DSAP), disseminated superficial porokeratosis (DSP), porokeratosis palmaris et plantaris disseminata (PPPD), punctate porokeratosis (PP), linear porokeratosis (LP)
Synonyms
Inclusive term “porokeratosis” may be used to refer to any or all of the various distinct clinical variants of porokeratosis
Definitions
Genodermatosis with clonal keratinocytic proliferation resulting in a clinically and morphologically distinct keratinization disorder
Hyperkeratotic plaques or papules surrounded by centrifugally expansile, thread-like, raised border that results in characteristic cornoid lamella
Several clinical variants of porokeratosis with overlapping features exist among described varieties
Classic variant: Porokeratosis of Mibelli
Common disseminated variants: Disseminated superficial actinic porokeratosis and disseminated superficial porokeratosis
Rare variants: Porokeratosis palmaris et plantaris disseminata, linear porokeratosis, localized porokeratosis, punctate porokeratosis, CAP syndrome, reticulate form, and many others
ETIOLOGY/PATHOGENESIS
Developmental Anomaly
Genetically heterogeneous condition that may be familial and tends to be inherited in autosomal dominant manner
Fully penetrant by 4th decade of life
Pathogenetic mechanisms are still somewhat unclear
Multiple current proposed concepts of pathogenetic mechanisms
Loci at chromosome bands 12q23.2-24.1 and 15q25.1-26 (DSAP1 and DSAP2) described in familial disseminated superficial actinic porokeratoses
Locus at DSAP1 corresponds to SART3, a candidate gene encoding a tumor rejection antigen and felt to be involved in regulation of mRNA splicing
SART3 mutations may thus result in altered proliferation and transformation of epithelial cells
Locus identified for disseminated superficial porokeratosis (DSP) at 18p11.3
Centrifugal expansion of cornoid lamellae in lesions may reflect migration of mutant clone of keratinocytes based on DNA ploidy and chromosome abnormalities
Higher prevalence of porokeratosis in immunosuppressed patients suggests impaired immunity, which permits disease in genetically predisposed
CAP syndrome (craniosynostosis, anal anomalies, and porokeratosis) is a rare genodermatosis found in only a few ethnically diverse families so far
Main phenotypic features are craniosynostosis and clavicular hypoplasia, anal anomalies, and widespread, small porokeratotic papules affecting face and extremities starting at 1 month of age
CLINICAL ISSUES
Epidemiology
Incidence
Relatively common pathological process
Disseminated superficial actinic porokeratosis is most common clinical variant
Age
Classic porokeratosis of Mibelli and rare linear porokeratosis variant begin during infancy or childhood with expansion of lesions in adulthood
DSAP and DSP variants often develop during 3rd or 4th decade of life
Porokeratosis palmaris et plantaris disseminata and punctate porokeratosis variants appear during adolescence and early adulthood
Gender
Porokeratosis of Mibelli and porokeratosis palmaris et plantaris disseminata show male predilection
DSAP and DSP both show female predilection: F:M = 3:1
Site
Distribution and site of lesions varies depending on clinical variant of porokeratosis
Porokeratosis of Mibelli develops as one or more round to oval plaques unilaterally on extremities
DSAP is typically widely distributed symmetrically over sun-exposed areas of extremities, with rare facial involvement and usual sparing of palms, soles, and mucous membranes
DSP occurs symmetrically on extremities similar to DSAP, but sun-protected areas are not spared
Presentation
Asymptomatic (occasionally pruritic), persistent, annular plaques or papules with characteristic circumferential, raised, hyperkeratotic ridge (rim) at periphery corresponding to cornoid lamella
Porokeratosis of Mibelli
Manifests as one or more asymptomatic, large, round to oval, skin-colored, red to brown, annular plaques often occurring unilaterally on extremities
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


