Plication of Perforated Duodenal Ulcer
Small anterior perforations of duodenal ulcers are treated by Graham patch plication, which may sometimes be performed laparoscopically (see Chapter 52). Larger perforations may require excision and closure by pyloroplasty or gastric resection for control.
In this chapter, the anatomy of the subhepatic space and its contents is introduced. The subphrenic spaces, frequent sites of associated abscess formation, are also demonstrated.
SCORE™, the Surgical Council on Resident Education, did not classify plication of perforated ulcer.
STEPS IN PROCEDURE
Upper midline or right paramedian incision
Explore and cleanse entire abdomen, especially subphrenic spaces and pelvis
Elevate liver and expose duodenum, suction away contamination
Visualize perforation; consider Graham patch only if perforation is small and anterior
Identify and, if necessary, mobilize tongue of omentum that reaches comfortably to perforation
Suture omentum over perforation using interrupted 2-0 silks
Irrigate abdomen and close
HALLMARK ANATOMIC COMPLICATIONS
Failure of seal (hole too large)
LIST OF STRUCTURES
Liver
Coronary ligament
Triangular ligaments
Falciform ligament
Ligamentum teres
Left and right subphrenic spaces
Subhepatic space
Lesser sac
Duodenum
Greater omentum
Gastroepiploic vessels
Identification of Perforation Site (Fig. 59.1)
Technical Points
Enter the abdomen through an upper midline or right paramedian incision (Fig. 59.1A) and thoroughly explore the abdomen. Often the site of perforation will have been sealed off by the overhanging liver and the omentum. Leave this seal undisturbed as you explore the left subphrenic space (over the stomach and spleen), the right subphrenic space (over the dome of the liver), and the rest of the abdomen. Culture the peritoneal fluid and remove as much contamination as possible by irrigation and suction. Then gently elevate the liver to expose the duodenum.
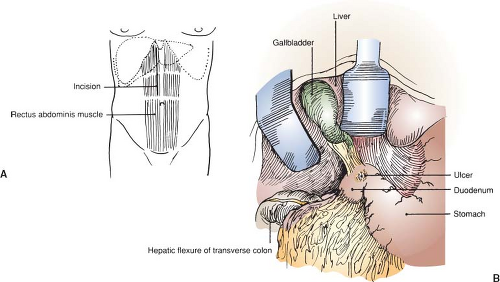 Figure 59.1 Identification of perforation site. A: Incision. B: Typical site of perforation. |
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


