Peritoneal Lavage: Insertion of a Peritoneal Dialysis Catheter
Peritoneal lavage is a diagnostic maneuver in which a catheter is inserted into the peritoneal cavity and fluid is aspirated. The character of the fluid (presence of blood, bile, or food particles, and its odor) is noted. If no fluid is obtained, 1 L of Ringer’s lactate solution is instilled, allowed to equilibrate with any fluid in the peritoneal cavity, and then aspirated. Although peritoneal lavage has largely been superseded by other diagnostic modalities such as FAST (focused abdominal ultrasound for trauma; see Chapter 40) or computed tomography scan, the procedure is still indicated under special circumstances.
A temporary or permanent peritoneal dialysis catheter is placed for peritoneal dialysis in patients with acute or chronic renal failure.
In this chapter, placement of a catheter for diagnostic peritoneal lavage is discussed first, followed by a description of the modifications necessary for placement of a permanent catheter. This procedure is used to introduce the anatomy of the anterior abdominal wall and the topography of the peritoneal recesses.
Steps in Procedure—Diagnostic Peritoneal Lavage
Lower midline incision (modified if previous scars)
Careful hemostasis as fascia is identified
Identify and lift up peritoneum
Create small incision and insert catheter, directing it toward the pelvis
Place purse string suture if desired
Confirm entry into peritoneum by free flow of intravenous fluid through catheter
Aspirate—free blood or succus indicates positive tap
Otherwise, instill 1 L Ringers lactate or normal saline and allow to dwell
Place bag on floor and submit effluent for laboratory analysis
Steps In Procedure—Placement of Tenckhoff Catheter
Access peritoneal cavity through small paramedian incision
Place small pursestring suture in peritoneum
Insert catheter, using guidewire if necessary to direct it to the pelvis
Position with one cuff in subcutaneous tissues, second cuff just superficial to the peritoneum
Tie pursestring suture and close incision
Hallmark Anatomic Complications
Preperitoneal catheter placement
Injury to bowel during access of peritoneum or placement of catheter
List of Structures
Linea alba
Umbilicus
Rectovesical pouch
Rectouterine pouch (of Douglas)
Pyramidalis muscle
Rectus Abdominis Muscle
Rectus sheath
Pubis
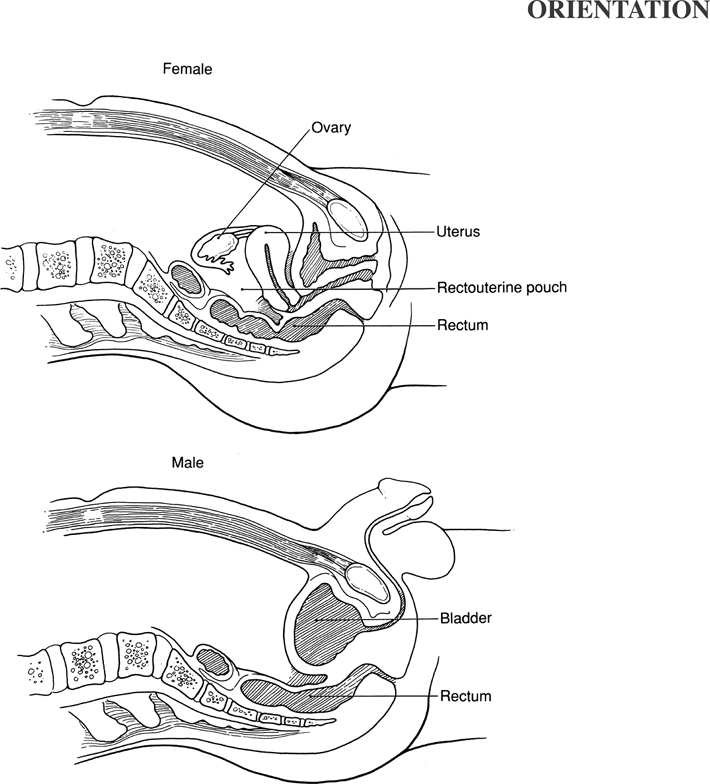 |
Diagnostic Peritoneal Lavage: Choice of Site (Fig. 39.1)
Technical Points
Note any scars from prior abdominal surgery. Because intraperitoneal adhesions form most densely on the underside of old scars, avoid such areas. In the absence of old scars or pelvic fractures, the preferred site is the lower midline, about 4 to 5 cm below the umbilicus. Alternative sites include the upper midline (for patients with pelvic fractures) and right lower quadrant. Ensure that the patient’s bladder is empty by having the conscious, cooperative patient void or by placing an indwelling Foley catheter. Shave, prepare, and infiltrate the area of the proposed skin incision. The use of lidocaine with epinephrine minimizes bleeding into the incision and may decrease the chance of a false-positive result. Careful hemostasis throughout the procedure is important.
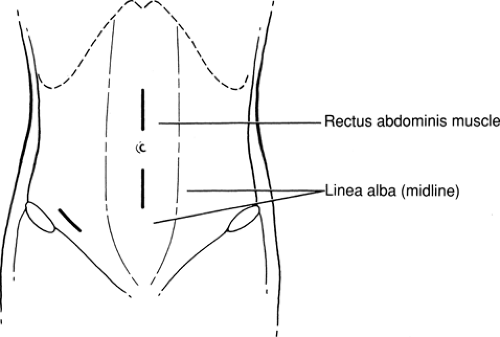 Figure 39-1 Diagnostic Peritoneal Lavage: Choice of Site
Stay updated, free articles. Join our Telegram channel
Full access? Get Clinical Tree
 Get Clinical Tree app for offline access
Get Clinical Tree app for offline access

|