Percutaneous Femoral-Popliteal Reconstruction Techniques: Antegrade Approaches
F. Gallardo Pedrajas
Peter A. Schneider
DEFINITION
Overview: Femoral-popliteal revascularization, for indications of limb salvage or claudication, is performed using open, endovascular, or hybrid approaches. Advanced open surgical techniques are detailed elsewhere. Guidewirecatheter combinations are particularly effective and widely used to cross femoral-popliteal stenoses or occlusions. Once across, reconstructions are performed with any combination of angioplasty, stenting, stent grafting, or atherectomy.
Basic procedural goals: Improve functional status, quality of life, and, in the setting of ischemic tissue loss, augment wound healing and limb preservation.
Challenges influencing long-term clinical success: (1) superficial femoral and popliteal artery movement during activities of daily living, including flexion, compression, torsion, and stretching; (2) compromised runoff; (3) the generally diffuse nature of femoral-popliteal disease, requiring angioplasty of long segments of diseased and stiffened artery; (4) complex pathology, including ostial lesions, luminal thrombus accumulation, and mural calcification.
Indications for intervention:
Rutherford class 1, 2, and 3 ischemia—exercise therapy and medical management are pursued as primary intervention.1
Rutherford class 4, 5, and 6 ischemia—rest pain, ischemic ulcer, and gangrene warrant revascularization as initial therapy.
Technical approach: Utilization patterns are trending toward percutaneous-first approaches to management of Inter-Societal Consensus for the Management of Peripheral Arterial Disease (TASC II) type A, B, and C lesions.2 Full consideration of current indications for open versus percutaneous interventions is beyond the scope of this text; reference should be made to most recent TASC updates.3
PATIENT HISTORY AND PHYSICAL FINDINGS
History includes a detailed description of ischemic symptoms pertaining to claudication, rest pain, or tissue loss. The progression of symptoms and timeframe are helpful in determining the urgency of therapy.
The presence and severity of cardiovascular disease risk factors should be assessed and managed to ensure optimal perioperative and long-term clinical results, including tobacco use, diabetes, hypertension, hyperlipidemia, renal dysfunction, and sedentary lifestyle.
Previous vascular or endovascular surgery procedures should be reviewed in detail, including obtaining operative notes, prior imaging and surveillance studies, and prior physiologic testing results whenever possible.
For claudicants, the potential presence and contribution of nonvascular causes of leg pain with exercise should be considered; for example, neurologic claudication secondary to lumbar radiculopathy and other degenerative spine diseases.4
Physical examination should document peripheral pulses at all levels, both lower extremities, including the strength and quality of femoral pulses and skin integrity at potential access sites.
The severity and extent of ischemia, degree of existing tissue damage, and presence of infection are documented prior to initiating intervention.
IMAGING AND OTHER DIAGNOSTIC STUDIES
Physiologic vascular testing provides objective determination of the location and severity of disease, assists in procedural planning, and provides documentation of baseline conditions.
Ankle-brachial index (ABI): ratio of the continuous wave Doppler-determined blood pressure in the anterior or posterior tibial arteries (whichever is higher) to the blood pressure in the brachial artery (>0.9 = normal; 0.5 to 0.9 = usually consistent with mild to severe claudication; <0.5 = present in patients with very short distance claudication, rest pain, or tissue loss)
Toe pressures: The ABI may be artifactually elevated in diabetic patients with calcified tibial arteries. Toe pressures may provide more reliable assessment of pedal and forefoot perfusion when the ABI is greater than 1.2. Hallux pressure less than 50 mmHg may predict delayed or inadequate wound resolution, 50 to 80 mmHg is indeterminant, and greater than 80 mmHg is generally sufficient to promote healing.
Duplex arterial imaging: Direct insonation provides insight into the location and severity of disease. The ratio of the peak systolic velocities (PSV) obtained from the most compromised location divided by PSV from the most adjacent, proximal noninvolved segment provides additional guidance regarding the severity of disease; greater than or equal to 2.5:1 usually identifies a stenosis greater than 50% (FIG 1).
Computed tomographic arteriography (CTA): CTA has assumed an increasing role in guiding peripheral vascular intervention, particularly in regard to choosing appropriate devices and optimal interventional approach (e.g., ipsilateral antegrade vs. contralateral retrograde). This additional guidance, however, comes at the cost of substantially more iodinated contrast and radiation exposure than that provided by catheter-directed, intraarterial contrast arteriography, augmented by direct ultrasonic visualization and physiologic testing (FIG 2).
Magnetic resonance arteriography (MRA): MRA may also assist preoperative planning. Although MRA does not expose patients to ionizing radiation, artifactual overestimation of disease severity is common in low flow conditions. Also, gadolinium contrast administration is contraindicated in patients with a glomerular filtration rate of less than 30 mL per minute due to risk of contrast-associated glomerulosclerosis (FIG 3).
SURGICAL MANAGEMENT
Overview—Success in percutaneous management of femoral-popliteal occlusive disease has catalyzed a reciprocal decline in the use of open bypass for definitive revascularization. Key features of percutaneous management include detailed preoperative planning, choice of access site and closure techniques, and familiarity and facility with a wide range of complementary intraluminal wire-guided devices.4
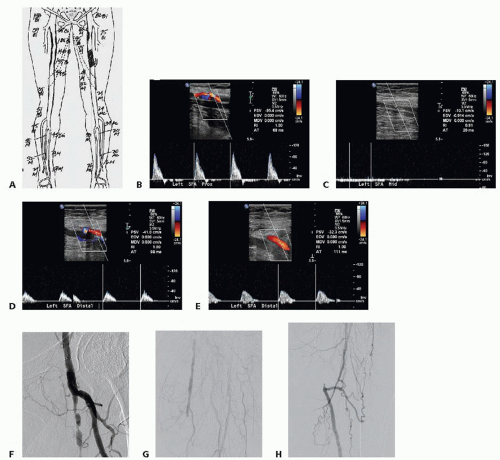 FIG 1 • Duplex evaluation of lower extremity arteries. A. Duplex mapping was performed on a patient with very severe left lower extremity claudication. There is a left SFA occlusion with reconstitution of the distal SFA. B. Duplex image of proximal left SFA shows some plaque formation and a peak velocity of 95 cm per second. C. This duplex image demonstrates no flow in the occluded segment of the SFA. D. The left distal SFA duplex image shows the point of reconstitution of the artery with a patent distal artery and low velocity flow. E. The more distal SFA is a healthier artery with a reasonable lumen, but it has a low peak velocity of 32 cm per second. F. The arteriogram performed on the left lower extremity of this patient at the time of intervention showed a patent but diseased proximal SFA. The CFA and profunda femoris artery do not have significant occlusive disease. G. There is a mid-SFA occlusion as demonstrated by duplex evaluation. H. There is reconstitution of the left distal SFA as indicated by duplex mapping. |
Preoperative Planning
The operative plan includes access site selection, planned method of crossing, and options for arterial reconstruction.
Endovascular inventory: An essential element of endovascular success is a robust and redundant device inventory. In contrast to open reconstruction techniques, where similar instruments will suffice for all lower extremity bypass configurations, regardless of routing, a unique and task-specific
repertoire is required for almost every endovascular approach. Procedural success requires that the necessary devices, including guidewires, sheaths, catheters, angioplasty balloons, stents, reentry devices, stent grafts, and atherectomy catheters are identified and available before intervention is attempted.
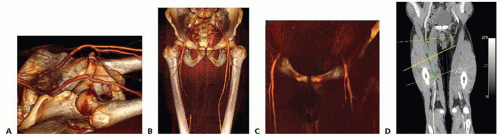
FIG 2 • CT angiography for infrainguinal occlusive disease. Volume rendering technique. Preoperative study of puncture zones in the CFA in a patient with a long right SFA occlusion. A. Evaluation of iliac artery inflow. B. Long right SFA occlusion with reconstitution of the above-the-knee popliteal artery. C. CT evaluation of the CFAs and femoral bifurcations prior to access. D. Centerline measurements performed to measure diameters and plan for stent graft placement in the right SFA.
Appropriate radiation protection must be available for all individuals involved in interventional procedures. All team members must conscientiously wear a radiation dosimeter, submitted monthly for aggregate exposure documentation. Leadership ensures that all team members adhere to basic radiation safety tenants, including limiting the length and intensity of exposure to the minimum required for precision imaging and intervention (the “as low as reasonably achievable” [ALARA] principle). Safety principles, including distance from the radiation source, appropriate shielding and optimal table height, and source-image intensifier distance, must be understood and applied during every procedure.
Antibiotic prophylaxis is administered prior to the initiation of the procedure, whenever permanent implants are considered.
Percutaneous procedures are performed under local anesthesia with appropriate sedation. Care should be taken to avoid oversedation to ensure that patients can cooperate with instructions and imaging requirements during the procedure. When hybrid open endovascular procedures are contemplated, general anesthesia may facilitate more rapid and accurate device deployment, with reciprocally less radiation exposure for the patient, cath lab team, and operator.
An important initial consideration is the approach and optimal puncture site. The common femoral artery (CFA) is the most frequent access site. The approach is typically either up and over the aortic bifurcation from the contralateral femoral artery or ipsilateral antegrade femoral puncture. The transbrachial, transthoracic approach may also provide optimal antegrade access under certain circumstances.
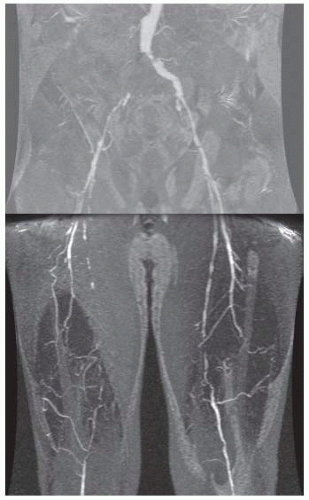 FIG 3 • Magnetic resonance angiography as preoperative assessment of lesion location and severity. This patient has extensive iliac and femoral artery occlusive disease. Both femoral artery puncture sites are compromised. There are long lesions in both superficial femoral arteries. |
Positioning
Surgeon position should provide forehand access, whenever possible (FIG 4).
Retrograde femoral puncture: This is the most common type of access for all endovascular procedures, including femoral-popliteal revascularization (FIG 5). The needle is placed in the CFA and the guidewire is advanced retrograde into the iliac artery.
The femoral area is examined prior to puncture of the artery. The inguinal ligament extends from the anterior superior iliac spine to the pubic tubercle. The best puncture
site is inferior to the inguinal ligament and at least a centimeter superior to the femoral bifurcation. Ultrasound provides useful guidance for arterial puncture (FIG 6). Following needle insertion, spot fluoroscopy from an ipsilateral oblique angle is obtained to confirm position. If arterial insertion is determined to be proximal to the femoral head, the access attempt is aborted before larger devices are inserted to minimize the risk of retroperitoneal hematoma formation due to inadequate compression or control following the procedure. Common femoral access also enables closure devices to be employed with confidence when necessary.
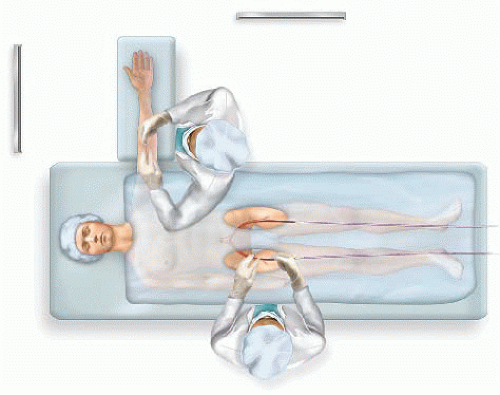
FIG 4 • Patient positioning. The operator works forehand when possible. The right-handed operator stands on the patient’s right side for a retrograde femoral puncture of either groin. The right-handed operator stands at the inferior aspect of the left arm when performing a left brachial puncture. The monitors are placed so that they can be comfortably observed by the operator.
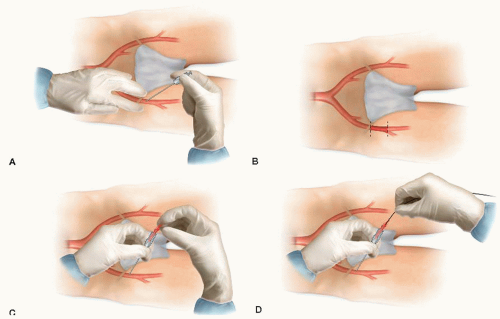
FIG 5 • Retrograde femoral puncture. A. The anatomic relationships are evaluated. The left hand may be used to help guide the needle. B. The access needle is placed in the CFA inferior to the inguinal ligament and superior to the femoral bifurcation. C. The needle is advanced into the CFA until arterial blood return is apparent. D. In the image a prolongation of the guide inside the retrograde femoral should be included, in order to understand that with this approach and these needle angulation the guide should never go to the SFA, or profunda artery.
Closure devices: recommended for retrograde femoral access site management following insertion of greater than or equal to 6-French (Fr) sheaths. Sheath puncture less than 6 Fr is best managed by compression for 10 to 15 minutes, with or without adjuncts such as a thrombin-impregnated dressing (e.g., D-stat® patch).
When pulses are not palpable at the desired access site, ultrasound or fluoroscopic guidance (assisted by mural femoral artery calcification) may provide valuable assistance. Under these circumstances, bilateral femoral access and ipsilateral iliac intervention may be required for procedural success. Ideally, this eventuality is anticipated based on the results of preprocedural examination and physiologic testing. Fortunately, the pulseless femoral artery is often palpable based on mural calcification alone. Patience and spot fluoroscopic images to confirm needle and artery position following failed needle passes often ensures ultimate success.
Secondary puncture of the postoperative groin presents special challenges. Whenever possible, scar tissue and anastomoses should be avoided. Access in native artery is preferable to prosthetic or autogenous grafts. Considerable force may be required for needle and micropuncture set access; consideration should be given to using “stiff” 0.018-in wires and
micropuncture sets specifically manufactured to facilitate difficult groin access.
Antegrade femoral puncture: The femoral pulse and inguinal ligament are carefully marked (FIG 7). Needle placement is directed proximal to the femoral artery bifurcation under real-time ultrasound guidance.
Guidewire placement into the superficial femoral artery (SFA) requires patience and practice. Ultrasound imaging in a longitudinal view may facilitate SFA wire intubation. When using a micropuncture set with a “steerable” 0.018-in wire (e.g., one with a slight curve placed at the tip), fluoroscopic control may also be employed. If repeated attempts result in deep femoral artery placement, the micropuncture set should be exchanged for an 11 cm 4- or 5-Fr sheath over a standard multipurpose (e.g., Bentsen) wire. Once safe antegrade deep femoral access is obtained, the 5-Fr sheath may be gradually withdrawn with sequential fluoroscopic contrast “puffs” of 1 mL or less performed until the femoral bifurcation is imaged (but while the sheath tip is still in the CFA). At this juncture, roadmapping or last-image-hold digital subtraction angiography from an ipsilateral oblique angle is performed to outline femoral bifurcation anatomy, after which a steerable hydrophilic guidewire and, ultimately, the 5-Fr sheath is directed under fluoroscopic imaging into the SFA.
Antegrade femoral access should be avoided in the obese, in patients with a short CFA, or in patients with extreme proximal or orificial SFA disease. Although antegrade access improves “pushability” across total occlusions and enables usage of a wider inventory of guidewire-catheter combinations, there is no option for inflow disease management using this approach. Also, the safety of current generation closure device placement is uncertain in antegrade approaches and should be avoided whenever possible.
Brachial puncture and transaortic sheath placement may provide an alternative option for “antegrade” femoral access. Upper extremity arteries are smaller, less forgiving, more prone to spasm, and less predictably managed with compression following access. Notoriously, small amounts of arterial extravasation may catalyze debilitating and permanent neurapraxia, even when brachial access is obtained well distal to the axillary fossa. Debilitating nerve injury from “axillary” sheath hematomas may occur at any location proximal to the antecubitum. In our practice, we minimize this risk by defaulting to surgical exposure and direct arterial puncture with suture closure for essentially all brachial artery access procedures. Exposure is easily obtained with local anesthetic in most patients.
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


