Operations on the Ureteropelvic Junction
Frank Hinman Jr.
As an alternative to open operation, consider endoscopic incision. If open surgery is indicated, the most adaptable technique is the Anderson–Hynes dismembered pyeloplasty. This method not only uniformly provides a funnel, but also allows resection of functionless portions of the pelvis and ureter. For selected cases, the YV-plasty and pelvic flap operations are excellent, whereas intubation techniques are reserved for cases in which more plastic methods are not possible.
Anderson–Hynes Dismembered Pyeloplasty
Expose the kidney through an anterior subcostal incision, taking care to stay out of the peritoneal cavity, or use a flank incision. In infants, the pelvis may be readily approached through a dorsal lumbotomy incision.
Open Gerota’s fascia laterally to preserve the dorsal layer; its contained perinephric fat will be used later to cover the repair.
Dissect the ureter starting below the ureteropelvic junction, taking care not to interfere with the segmental blood supply to this area (Fig. 1). Place a small Penrose drain or vessel loop around the ureter.
After exposure of the ureteropelvic junction, decide on the type of operation. Ureteropelvic junction obstructions are usually from an anomalous insertion of the ureter, with or without stricture, from a stricture just below the ureteropelvic junction, or, in the upper ureter, from a stricture or a ureteral valve. Ask yourself: Is the ureter long enough to allow dismemberment and excision of the ureteropelvic junction? If so, a modified Anderson–Hynes pyeloplasty is suitable most often, although a Foley Y-plasty can work well with high insertions of the ureter. For a long dependent junction, the Culp or Scardino techniques may solve the problem of having insufficient ureter for approximation.
Place a stay suture in the ureter at its junction with the pelvis (Fig. 2), divide the ureter obliquely, and spatulate it on its (less vascularized) lateral surface for a distance equal to the length of the proposed V-shaped flap.
With the pelvis full, map the proposed diamond-shaped incision with a skin-marking pen, angling the caudal triangle medially to form a V-flap (Fig. 3). Place stay sutures of 7-0 catgut at the angles of the diamond. Incise along one of the planned lines for a short distance with a no. 11 hooked blade. With Lahey or Potts scissors, cut the pelvis from the inside of one stay suture to the inside of the next (Fig. 4).
Insert an infant feeding tube of suitable size into the ureter to prevent a suture from catching the far wall (Fig. 5). Place one 5-0 or 6-0 synthetic absorbable suture adjacent to the apex of the V-shaped flap, inserted first from outside in, then out through the apex of the ureteral slit. Place a second suture 2 mm away from the first. Tie both sutures with four knots and cut the short ends.
Continue the first suture along the far side of the wall to the tip of the ureter as a continuous stitch, locked at every four or five bites (Fig. 6A). Do the same for the second suture on the near side. Be sure to irrigate the pelvis and calices free of clots.
Tie the two sutures together, cut one at the knot, and close the pelvic defect with the other (Fig. 6B). If the infant feeding tube is to remain as a stent, bring it out through the renal parenchyma.
Inject saline with a fine needle through the pelvic wall to test for watertightness and for patency of the anastomosis.
Insert a Penrose drain and fasten it by the long-suture technique to be sure it is near but not touching the anastomosis or the ureter below it (Fig. 7). Nephropexy stitches can be used to hold the kidney in place if it has been mobilized. Tack the two edges of Gerota fascia together around the kidney with fine plain catgut to isolate the kidney from the body wall and close the wound in layers.
Foley Yv-Plasty
This technique may be indicated for a high insertion of the ureter, especially when the pelvis has a box shape (Fig. 8A).
Draw the ureter cephalad with a Penrose drain and mark a long Y-shaped incision between stay sutures. Incise the pelvis between the stays with a no. 11 hooked blade, and open it with Potts scissors. This forms a V with arms equal to the length of the ureteral incision (Fig. 8B). A nephrostomy tube may be placed, with or without a stent. Suture the apex of the flap to the apex of the ureteric incision with a 7-0 synthetic absorbable suture passed in through the apex of the V and out through the apex of the ureteral incision (Fig. 9A). Place interrupted sutures of 4-0 synthetic absorbable suture down both sides of the V to make a watertight anastomosis (Fig. 9B).
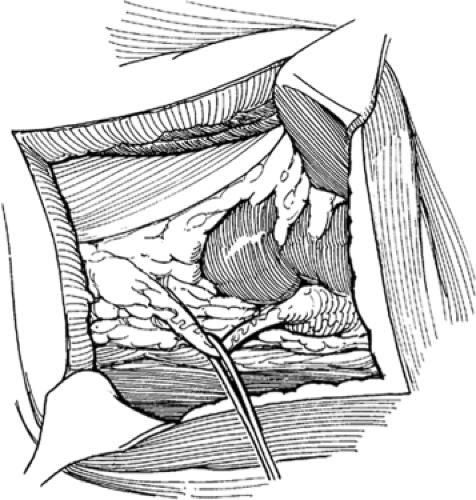 Fig. 1. Anderson–Hynes dismembered pyeloplasty. Exposure and dissection of the ureteropelvic junction. (From Hinman F Jr. Atlas of Urologic Surgery, 2nd ed. Philadelphia: WB Saunders, 1998, with permission.) |
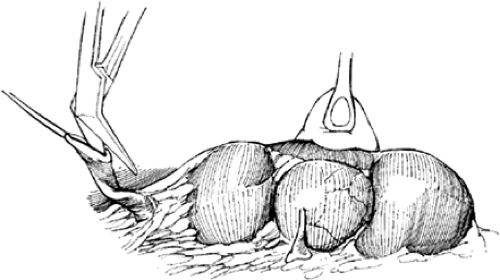 Fig. 2. Division and spatulation of the ureter. (From Hinman F Jr. Atlas of Urologic Surgery, 2nd ed. Philadelphia: WB Saunders, 1998, with permission.) |
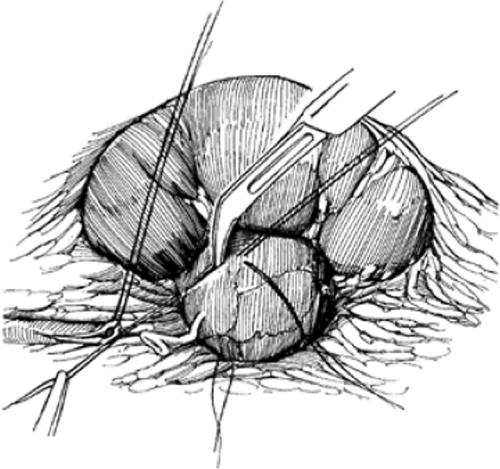 Fig. 3. Mapping and incising the pelvis. (From Hinman F Jr. Atlas of Urologic Surgery, 2nd ed. Philadelphia: WB Saunders, 1998, with permission.) |
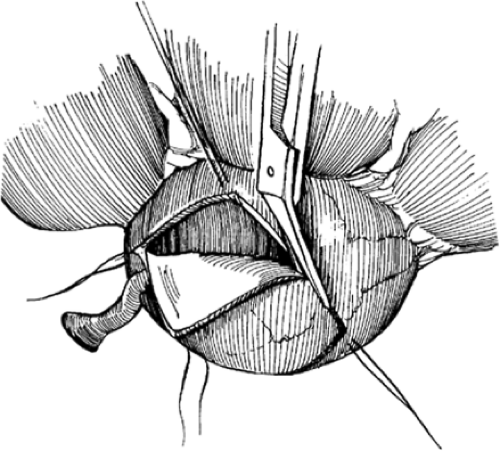 Fig. 4. Completing the pelvic incision–excision. (From Hinman F Jr. Atlas of Urologic Surgery, 2nd ed. Philadelphia: WB Saunders, 1998, with permission.)
Stay updated, free articles. Join our Telegram channel
Full access? Get Clinical Tree
 Get Clinical Tree app for offline access
Get Clinical Tree app for offline access

|