Operations for Small Bowel Obstruction
A dhesions are the most common cause of small bowel obstruction in the United States and other westernized countries. When adhesive small bowel obstruction fails to resolve with bowel rest and intravenous fluids, laparotomy or laparoscopy may be required. Surgery is generally required for the other causes (hernia, carcinoma, stricture). The first part of this chapter deals with open laparotomy for small bowel obstruction. The skills described here are also used whenever the abdomen must be opened after previous abdominal surgery. The chapter concludes with a discussion of laparoscopic lysis of adhesions.
SCORE™, the Surgical Council on Resident Education, classified open and laparoscopic adhesiolysis as “ESSENTIAL COMMON” procedures.
STEPS IN PROCEDURE
Open the abdomen through a site above or below the old incision if possible
If necessary, open through upper part of old incision
Carefully lyse adhesions to underside of abdominal wall
Lyse adhesions between loops of bowel
Identify the obstructive mechanism and release it
Consider side-to-side bypass in difficult situations
Choose a dilated proximal and collapsed distal segment
Ensure there is no additional obstruction downstream
Create sutured or stapled side-to-side anastomosis
Assess bowel for viability and injuries
Repair any injuries, resect nonviable bowel
Close incision in usual fashion
HALLMARK ANATOMIC COMPLICATIONS
Injury to bowel
Missed obstruction
LIST OF STRUCTURES
Small intestine
Jejunum
Ileum
Ligament of Treitz
Opening the Abdomen (Fig. 88.1)
If opening the abdomen after a previous midline incision, extend the incision into fresh territory cephalad or caudad if possible (Fig. 88.1A). Be sure that the incision will provide you with good access to the presumed point of obstruction on preoperative imaging studies. If the old incision extends from xiphoid to pubis, it is generally best to re-enter the abdomen through the upper aspect, where only the liver and stomach are likely to be encountered, rather than loops of small bowel.
If the previous incision was made elsewhere in the abdominal wall (e.g., a right lower quadrant incision for appendicitis), make a short midline incision near the likely site of obstruction.
Elevate the abdomen by lifting up strongly on the incision on your side (and have your assistant lift up opposite to you) and enter the peritoneal cavity with care, using scalpel (see Chapter 44). Be aware that adhesions tend to form to suture material, so there are often dense adhesions to the underside of the incision. In extreme cases, entering the abdomen just lateral to a dense adhesion (Fig. 88.1B) and allowing a small nubbin of fascia to remain adherent to a loop of bowel may prevent enterotomy. This nubbin can then be debrided during the enterolysis part of the operation.
Once a clear window has been formed, it may be possible to open the fascia with cautery in the usual fashion. Be aware
that a collapsed loop of bowel may be adherent to the inferior aspect of the incision where it is easily mistaken for peritoneum and injured during entry.
that a collapsed loop of bowel may be adherent to the inferior aspect of the incision where it is easily mistaken for peritoneum and injured during entry.
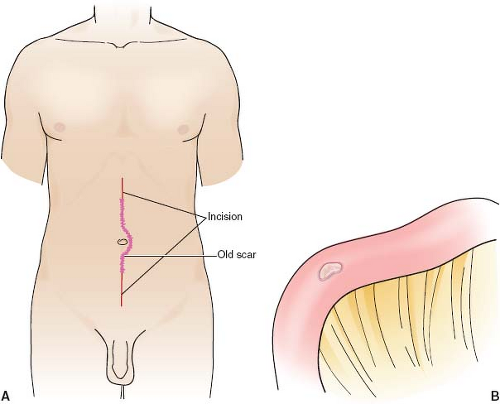 Figure 88.1 A: Enter the abdomen through a fresh area above or below the old incision. B: Leave a small nubbin of fascia adherent to the bowel to avoid injuring the bowel. |
Enterolysis and Identification of Site of Obstruction (Fig. 88.2)
First, concentrate on lysing adhesions of bowel to abdominal wall. Have your assistant elevate the abdominal wall by pulling on Kocher or Allis clamps placed on the fascial edges and carefully take down the adherent loops of bowel with Metzenbaum scissors or scalpel, insinuating your hand behind each loop of bowel if possible. Gentle downward traction on the loop will then usually reveal the adhesion that needs to be divided (Fig. 88.2A). In most cases, the adhesions become less dense as the dissection progresses away from the incision. Once the block of small intestine has been freed from the abdominal wall, place fixed retractors.
It is prudent to keep the area you are working upon isolated with laparotomy pads, and to have a Yankauer suction close at hand. Inadvertant enterotomy during dissection may result in copious spillage of the liquid contents of the obstructed bowel.
Next, lyse adhesions between loops of bowel by similarly insinuating your finger behind the adhesion and displaying it for division with electrocautery or Metzenbaum scissors (Fig. 88.2B). At all times be alert for the point of obstruction. If the preoperative imaging studies showed a clear transition between proximal dilated bowel and distal collapsed bowel, then a discrete point of obstruction (often a single adhesive band) will be found. Carefully inspect the bowel at the site of obstruction for viability; in extreme cases, pressure from the obstructing band will have caused localized necrosis (in a ring-like fashion) of the trapped bowel. Continue to lyse all adhesions from the ligament of Treitz to the ileocecal valve.
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


