Open Drainage of Abdominal Abscesses
Most intra-abdominal abscesses are now managed by image-guided percutaneous drainage and antibiotics. Open drainage is used when percutaneous drainage fails or is not available, or when abscesses are encountered during open surgery. Access for open drainage may be obtained transperitoneally or extraperitoneally.
Extraperitoneal drainage is primarily used to drain an isolated abscess, such as an isolated subphrenic abscess. The major advantage is that the peritoneal cavity is not violated; this is, in fact, also the drawback of this approach. The abdomen cannot be explored and any underlying cause of the abscess cannot be addressed. Most abscesses that would have been amenable to extraperitoneal drainage are now managed percutaneously.
Transperitoneal drainage is used when there are multiple abscesses or an underlying problem (such as a perforation or anastomotic leak) must be addressed surgically.
This chapter demonstrates the recesses of the peritoneal cavity, a concept introduced in Chapter 42, and describes transperitoneal and extraperitoneal approaches to several common types of abscess. References at the end discuss management of less common kinds of abscesses, and Chapter 87 discusses drainage of infected pancreatic sequestrums.
SCORE™, the Surgical Council on Resident Education, classified open drainage of abdominal abscess as an “ESSENTIAL UNCOMMON” operation.
STEPS IN PROCEDURE
Intraperitoneal drainage of subphrenic abscess
Explore the abdomen
Place retractors to expose the right upper quadrant
Explore the line of adhesion between free edge of liver and diaphragm
Gently mobilize the liver down from the diaphragm
Take care to avoid entering the capsule of the liver
Have suction ready to deal with pus
Enter and explore the subphrenic space
Culture purulence
Break down loculations
Irrigate and place drains
Extraperitoneal Drainage—Anterior Approach
Incision 2 cm below and parallel to costal margin
Enter extraperitoneal space
Gently mobilize peritoneum downwards
Aspirate through peritoneum to identify abscess
Enter abscess and proceed as above
Extraperitoneal Drainage—Posterior Approach
Lateral position
Incision over twelfth rib
Elevate periosteum from rib and resect it
Push pleural reflection cephalad
Develop the extraperitoneal space
Aspirate to identify the abscess, and proceed as above
HALLMARK ANATOMIC COMPLICATIONS
Injury to liver
Missed second abscess
Injury to intercostal nerves
Inadvertent entry into pleural space (posterior approach)
LIST OF STRUCTURES
Liver
Diaphragm
Peritoneum
Twelfth rib
Eleventh and twelfth intercostal nerves
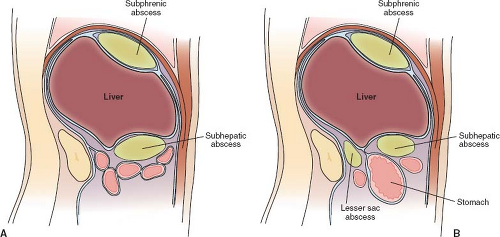 Figure 45.1 A: Potential spaces for abscess formation in the upper abdomen on the right include the very large right subphrenic and right subhepatic spaces. B: Potential spaces on the left include a left subphrenic, left subhepatic space (anterior to the stomach), and lesser sac (posterior to the stomach). |
In the upper abdomen, there is a space between the underside of the diaphragm and the diaphragmatic surface of the liver, termed the right and left subphrenic spaces. Suction during inspiration draws fluid from anywhere in the abdomen into this space, where it is normally cleared by diaphragmatic lymphatics. This suction effect explains how abscesses can form in these spaces after infectious processes in the lower abdomen. The right side has the large right subphrenic space (Fig. 45.1A) and a subhepatic space. On the left, there is a smaller left subphrenic space and a subhepatic space. There is also a space in the lesser sac (Fig. 45.1B). In the mid abdomen, abscesses may form along the lateral gutters or between loops of bowel (termed interloop abscesses). In the pelvis, abscesses form in the deep recesses between the rectum and bladder (in the male) and the rectum and uterus (in the female).
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


