Oncoplastic Techniques in Breast Surgery
Oncoplastics is a term used to describe the application of plastic surgical techniques to cancer surgery of the breast. This chapter describes the use of two oncoplastic techniques to resect large areas of the upper or lower aspect of the breast with subsequent re-creation of the breast shape. Often a corresponding procedure must be done on the other side to achieve symmetry.
This chapter also describes some considerations for skin and nipple-areolar complex sparing mastectomy.
SCORE™, the Resident Council on Surgical Education, does not classify these procedures.
STEPS IN PROCEDURE
Oncoplastic Resection Through Batwing Incision
Outline incision along upper aspect of areola
Draw medial and lateral transverse extensions
Create upper incision in similar fashion so that “batwing” of skin is excised with specimen
Raise flaps and excise specimen in usual fashion
Confirm adequacy of excision by specimen radiography or other means
Optional—mobilize remaining breast tissue at the level of pectoral fascia and reapproximate to eliminate dead space
Close incision in usual fashion
Oncoplastic Resection Through Education Mastopexy Incision
Outline incision with the assistance of plastic surgeon
Resect area of involvement and confirm adequacy of resection
Mark edges of the cavity with clips
Closure generally done by plastic surgeon
Skin-Sparing Mastectomy
Incision may be circumareolar, have a keyhole extension, or be modified to incorporate prior biopsy site
Develop cone of skin and subcutaneous tissue by dissecting circumferentially
Mobilize breast from underlying pectoral fascia
Obtain hemostasis and allow plastic surgeon to complete the procedure
Nipple-Areolar–Sparing Mastectomy
Incision may be lateral or inframammary (hockey stick)
Ducts are dissected off the nipple
Biopsy terminal ducts
Finish mastectomy as above
HALLMARK ANATOMIC COMPLICATIONS
Skin-flap necrosis (skin-sparing mastectomy)
Nipple necrosis (nipple-areolar–sparing mastectomy)
LIST OF STRUCTURES
Areola
Internal thoracic (mammary) vessels
Pectoral fascia
Cooper’s ligaments
Ribs
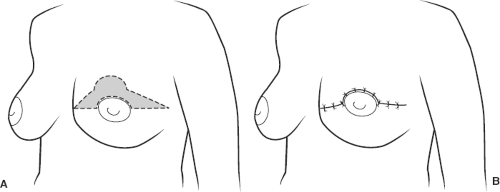 Figure 19.1 Oncoplastic resection—batwing incision. A: Incision. Note extent of skin resection. B: Result after resection and closure of incision. Note this will lift the operated breast; hence, a corresponding lift may be needed on the opposite side for symmetry. |
Oncoplastic Lumpectomy—Batwing Incision (Fig. 19.1)
Technical and Anatomic Points
This incision allows removal of a significant amount of tissue from the upper aspect of the breast. It is useful for excising large regions of ductal carcinoma in situ (DCIS) or for removal of large benign tumors such as giant fibroadenomas. When the incision is closed, the result is a breast that is slightly smaller and less ptotic than it was before surgery. Sometimes a similar re-excision will be performed on the opposite side to achieve symmetry.
Outline the incision by first defining the area of the tissue to be removed. Outline the upper aspect of the areolar boundary. Then draw medial and lateral extensions. Create the upper part of the incision in a similar fashion, outlining a contour that will naturally mate to the inferior aspect (Fig. 19.1A).
Elevate flaps and remove tissue as described for lumpectomy. Some surgeons will mobilize the breast tissue from the pectoral fascia and approximate it to eliminate the dead space. Close without drains (Fig. 19.1B).
Oncoplastic Resection—Reduction Mastopexy Incision (Fig. 19.2)
Technical and Anatomic Points
For a woman with relatively large, ptotic breasts, resection of large lesions in the inferior half of the breast may be combined with reduction mastopexy. Reduction mastopexy is usually done on the contralateral breast to re-establish symmetry.
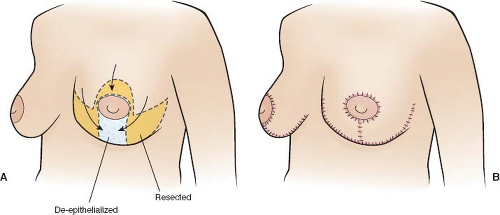 Figure 19.2 Oncoplastic resection—reduction mastopexy approach. A: Incision. B: Closure—note reduction on contralateral side for symmetry. |
The incision is shown in Figure 19.2A. Generally, the cancer surgeon performs the resection and assures adequacy of the excision. This may require needle localization, ultrasound, specimen radiograph, or any of the techniques in current use to maximize the chance of a negative margin. The plastic surgeon then reconstructs the shape of the breast by bringing the tissue together. This may require resection of additional tissue (which should be oriented and submitted for pathologic examination), elevation of flaps, and/or transposition of some tissue. For that reason, it is prudent to place marking clips in the excision bed before the reconstructive phase of this operation is performed.
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


