Obesity and the Eating Disorders
“You cannot be too rich or too thin.” This quote, often attributed to Wallace Simpson, the reed-thin American wife of the late Duke of Windsor, reflects the attitude of many Americans toward body weight. That is, they equate being thin with being successful, while being obese reflects laziness and lack of self-control. This idealized view of thin people and negative view of overweight people are significant contributing factors to the financial success of the American weight control industry and, unfortunately, to the high prevalence of eating disorders such as anorexia nervosa and bulimia nervosa in the U.S. population.
• OBESITY
Obesity is a common health concern in the United States. Between 25% and 50% of American adults are obese, and their numbers are increasing.
Characteristics
Obesity is defined as more than 20% over ideal weight based on insurance company standard height and weight tables. Body mass index (BMI), the ratio of body weight in kg to height in m2, may be a more accurate indicator of obesity than body weight. Normal BMI is in the range of 20 to 24.9 (Fig. 17-1). A BMI of 25 or higher indicates that an individual is overweight, and a person with a BMI of 30 or greater is considered obese.
The formula for calculating BMI is body weight in kg divided by height in m2. Using pounds, the formula is
BMI = Body weight (lb) × 705/height (inches)/height (inches)
The prevalence of obesity in the United States varies by ethnic group in women but not in men (Flegal et al., 2002) and is also more common in women than in men. The Samoans in Oahu, Hawaii, are the heaviest American group with 75% of the male and 80% of the female population described as obese. In children, the term overweight is used to describe excess body weight and is defined as at or above the 95th percentile of the sex-specific BMI for age growth charts. The prevalence of overweight children, which is increasing among children aged 2 through 19 years, is currently highest among Mexican-American and non-Hispanic African-American adolescents ages 12 to 19 years (Ogden et al., 2002).
Health problems associated with obesity include cardiorespiratory problems (e.g., hypertension) and increased risk for hypercholesteremia, cancer, diabetes, orthopedic problems, and early death. A specific disorder of obesity, Pickwickian syndrome, is characterized by a body weight more than twice that of normal, as well as respiratory (e.g., alveolar hypoventilation), cardiovascular, and sleep problems (see Chapter 7).
Etiology
Obesity is not an eating disorder. Many elements, including biological, social, and psychological factors, are involved in its etiology. There is a strong genetic component; adult body weight is closer to that of biological rather than of adoptive parents. Moreover, many obese patients have a family history of obesity. Mutations in at least two genes, the leptin receptor (LEPR) gene and the melanocortin 4 receptor (MC4R) gene, have been implicated in obesity (Branson et al., 2003; Farooqui et al., 2003; List & Habener, 2003). Endocrine disorders such as Cushing’s disease, hypothyroidism, and use of psychoactive agents such as antipsychotics and antidepressants are also associated with obesity.
Because physical activity is important in the maintenance of body weight, the sedentary lifestyle and reliance on automobiles of the mechanized American society are significant factors in the rising obesity rates. As evidence for this association, obesity and its associated complications are increasing in Asia as more of that population moves to large cities and becomes more sedentary (Mydans, 2003).
No specific psychological component has been associated with the development of obesity. In fact, the type and degree of psychopathology of overweight and obese people are quite similar to those of the typical-weight population.
No specific psychological component has been associated with the development of obesity. In fact, the type and degree of psychopathology of overweight and obese people are quite similar to those of the typical-weight population.
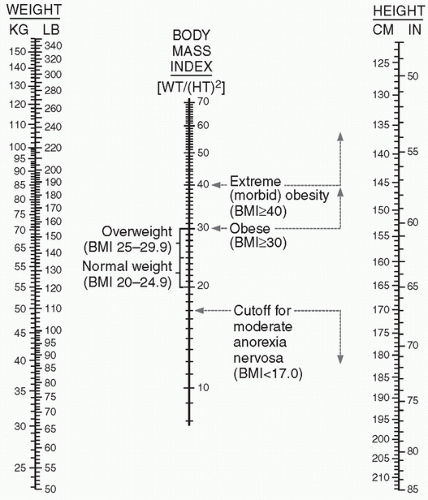 FIGURE 17-1. Body mass index (BMI). BMI is calculated by placing a straight edge between the body-weight column (left) and the height column (right) and reading the BMI from the point at which the straight edge crosses the BMI column. (Adapted from Bray GA. Definitions, measurements and classification of the syndromes of obesity. Int J Obes. 1978;2:99.) |
Management
Although many commercial dieting and weight loss programs are effective initially, most weight lost is regained within a 5-year period. Surgical techniques, that is, bariatric surgery such as gastric bypass (food is rerouted past part of the stomach and the small intestine) and gastric banding (the size of the stomach is effectively reduced), result in initial weight loss. A variety of serious sequelae, including vomiting, diarrhea, intestinal obstructions, electrolyte disturbances, and the well-documented problems associated with exposing obese patients to major surgery, limit the usefulness of these procedures. Whether such procedures are effective for lasting maintenance of body weight is not known, and they are usually employed only when less invasive strategies have failed.
Amphetamines such as dextroamphetamine decrease appetite and were once commonly used in weight loss programs. However, the abuse potential of these agents (see Chapter 23) has limited their utility, and they are now rarely prescribed for weight loss. The amphetamine-like agent phentermine (Ionamin), a sympathomimetic amine, is FDA approved only for short-term treatment of obesity. Related agents such as dexfenfluramine (Redux), fenfluramine (Pondimin), and sibutramine hydrochloride (Meridia) have been taken off the market because of their side effects. A newer, FDA-approved agent to be used long-term for weight-loss is orlistat (Xenical). Orlistat is not an appetite suppressant; it is a pancreatic lipase inhibitor that limits the breakdown of dietary fats, thereby decreasing their absorption by about one-third. This agent is also now available without prescription in a low dose formulation known as Alli. Although weight loss agents are indicated for weight loss in patients with BMIs greater than 30 (or greater than 27 in the presence of other risk factors, such as hypertension or diabetes), they can have negative
effects such as elevation of blood pressure (phentermine) and gastrointestinal problems (orlistat). Two anticonvulsants, topiramate (Topamax) and zonisamide (Zonegran), alone or in combination with other agents, also appear to have the potential to facilitate weight loss (Jones, 2009).
effects such as elevation of blood pressure (phentermine) and gastrointestinal problems (orlistat). Two anticonvulsants, topiramate (Topamax) and zonisamide (Zonegran), alone or in combination with other agents, also appear to have the potential to facilitate weight loss (Jones, 2009).
For most people, maintenance of weight loss is best achieved by a combination of sensible dieting and exercise tailored to the person’s capabilities. Typically, sensible dieting involves a low-calorie, high-carbohydrate, low-fat regimen (conventional diet). Recent preliminary studies indicate that when compared with a conventional diet, the low-carbohydrate, high-protein, high-fat (Atkins) diet may produce greater weight loss and more improvement in some risk factors for heart disease (Foster et al., 2003; Samaha et al., 2003). Twelvestep peer-support programs based on the Alcoholics Anonymous (AA) model (see Chapter 23) such as Overeaters Anonymous can also be helpful in long-term maintenance of weight loss.
• OVERVIEW OF THE EATING DISORDERS
Characteristics
Patients with eating disorders typically have normal appetites but show abnormal behavior associated with food. Anorexia nervosa and bulimia nervosa patients also often use compensatory mechanisms to avoid weight gain, such as vomiting and abuse of diuretics, enemas, and laxatives. This purging behavior can lead to malnutrition and electrolyte disturbances that can lead to serious cardiovascular problems, such as life-threatening arrhythmias. Recurrent laxative abuse may result in melanosis coli, a darkened area of mucosa identified during examination of the colon. This benign condition (the brown pigmentation is not melanin but lipofuscin in macrophages) is seen particularly in patients abusing laxatives that contain anthraquinone such as senna (Senocot) and other plant glycosides (Fig. 17-2). Patients with eating disorders may also use drugs or thyroid hormones to lose weight, or they may seek surgical procedures such as liposuction to remove body fat.
 FIGURE 17-2. Melanosis coli. Darkened area on the colon resulting from abuse of senna-containing laxatives. (Photo courtesy Gastrolab/Photo Researchers, Inc.) Patients with eating disorders tend to engage excessively in sports and strenuous exercise aimed at weight loss, behavior that has been called hypergymnasia. Gymnastics and ballet dancing in particular are seen in patients with these disorders, probably because they require that participants have low body weight. Characteristically, and despite normal or below normal body weight, eating disorder patients show disturbances of body image and often feel that they look “fat.” |
Occurrence
The eating disorders are more common in women; each occurs in about 1% to 3% of women and 0.1% to 0.2% of men. These disorders are more common in late adolescence and young adulthood and are more likely to be seen in high academic achievers and in higher socioeconomic groups. Prepubertal obesity and dieting, stressful life events such as sexual abuse, and having family members with eating disorders or substance abuse are risk factors for eating disorders. Table 17-1 compares the physical and psychological characteristics of anorexia nervosa and bulimia nervosa.
table 17.1 COMPARISON OF THE PHYSICAL AND PSYCHOLOGICAL CHARACTERISTICS OF ANOREXIA NERVOSA, BULIMIA NERVOSA AND BINGE-EATING DISORDER |
|---|



