Normal Cellular Components and Reactive Mesothelial Proliferations
Donna M. Coffey, MD
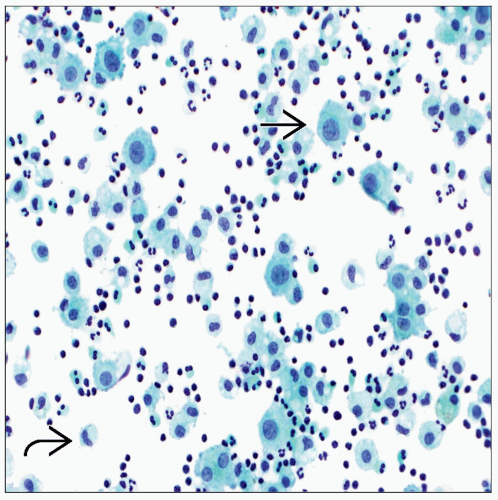 Pap stain shows a pleural effusion with a mesothelial cell  and a dispersed single-cell pattern, histiocytes and a dispersed single-cell pattern, histiocytes  , and inflammatory cells. Mesothelial cells have minimal variation in cell and nuclear size. , and inflammatory cells. Mesothelial cells have minimal variation in cell and nuclear size. |
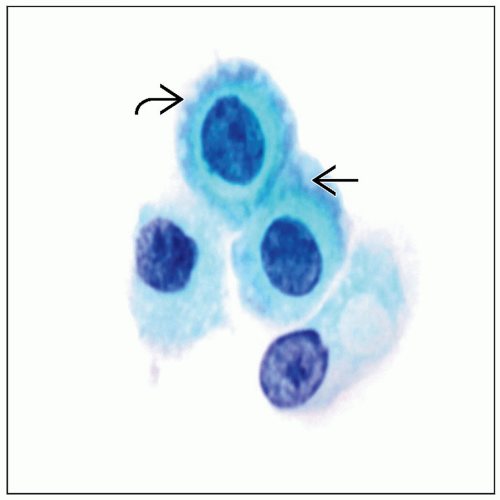 Pap stain of an effusion shows mesothelial cells with round nuclei and abundant cytoplasm. Long slender microvilli result in a peripheral clear zone “lacy skirt”  and intercellular windows and intercellular windows  . . |
GENERAL PRINCIPLES
Pleural, Pericardia, and Peritoneal Cavities
Lined by a single layer of mesothelial cells and underlying loose fibroconnective tissue
In normal conditions, serous cavities contain a minimal amount of fluid for lubrication of surfaces
Fluid is virtually acellular; contains rare mesothelial cells
Variety of conditions, including neoplastic and nonneoplastic, can result in an accumulation of fluid or effusion
Reactive mesothelial hyperplasia is often seen in association with infections, collagen vascular disease, drug reactions, pneumothorax, chest surgery, and trauma
Depending on physical, chemical, and microscopic characteristics of the fluid, effusions can be subdivided into transudates and exudates
Distinction is important because most malignant effusions are exudates; therefore, cytologic evaluation of transudates is not as critical
Transudates: Result of intravascular pressure alteration (CHF, nephrotic syndrome, cirrhosis)
Clear fluids with low specific gravity (< 1.015), low protein content (< 3 g/dL), and low lactate dehydrogenase (LDH) level (< serum LDH)
Have scant cellularity with rare mesothelial cells, histiocytes, and lymphocytes
Exudates: Result from mesothelium injury (malignancy, infections, autoimmune diseases, infarction, trauma)
Turbid fluids with greater specific gravity (> 1.015), high protein content (> 3g/dL), and high LDH level (> serum LDH)
Tend to have higher cellularity with numerous mesothelial cells, inflammatory cells, ± tumor cells
COLLECTION AND PROCESSING
Body Fluids
Collected by aspiration of cavities or by collection of pelvic washings at time of surgery
Specimens are collected and sent unfixed in heparinized bottles
Specimens are processed immediately or refrigerated at 4°C until time of slide preparation
Specimens may be processed as direct smears, cytocentrifuge slides, thin-layer slides, or filter preparation
Pap and Diff-Quik stains are used for routine cytology
Thrombin cell blocks can be prepared from the fluid
Cell block sections are useful to evaluate architecture and to perform immunocytochemical/special stains or molecular analysis
Fresh fluid can be submitted for flow cytometry, cytogenetics, or molecular analysis
Peritoneal washings are often collected during staging of gynecologic or other nongynecologic peritoneal malignancies or to rule out malignancy in a patient undergoing surgery for presumed benign condition
Peritoneal washings strip the mesothelial surface, resulting in large sheets of cells that can be folded, imparting a 3D appearance
Collagen balls and numerous histiocytes are often present
Because these specimens are collected as part of surgical staging, correlation with concurrent surgical specimen is recommended
NORMAL CELLULAR COMPONENTS
Benign Effusions
Contain variable numbers of mesothelial cells, histiocytes, lymphocytes, and red blood cells
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


