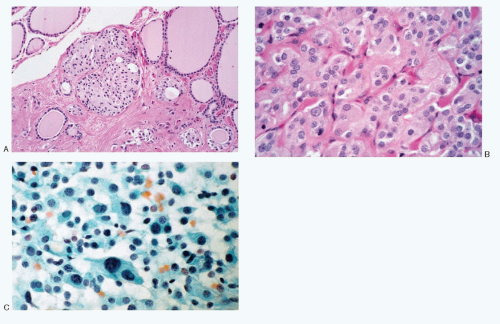
 Fig. 8.1: A: Histologic section of a thyroid demonstrating C-cell hyperplasia. Note well-defined nests of cuboidal to polygonal cells in between the thyroid follicles. There was no grossly visible tumor. The patient had several members of the family with hereditary type medullary carcinoma. B: Higher magnification. These cells have abundant eosinophilic cytoplasm. C: Imprint of the surgically resected specimen showing discrete C cells with plasmacytoid appearance. |
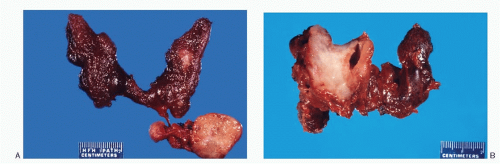 Fig. 8.2: A: A gross photograph of a nonfamilial (sporadic) form of medullary thyroid carcinoma located in the middle third of the left lobe and lymph node metastases (arrow). B: This nonfamilial medullary carcinoma is large replacing the entire right lobe. The tumor presents a flat cut surface. |
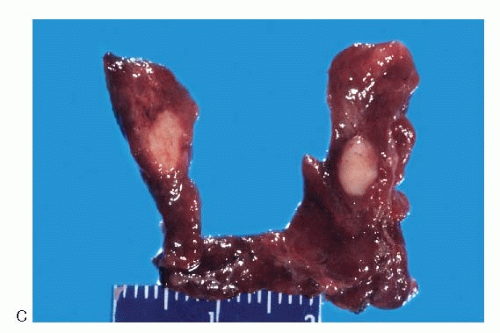 Fig. 8.2: (continued) C: An example of hereditary medullary carcinoma. Note the tumor is located in the middle third of the lobe and bilateral. |
TABLE 8.1. HEREDITARY FORMS OF MEDULLARY THYROID CARCINOMA | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| |||||||||||||||||||||||||||||||||||||||||||||||||||||||||
mucin. Their nuclei can be monomorphic to pleomorphic, round, oval, oblong to spindle shape with stippled to coarsely granular chromatin popularly referred to as salt-pepper chromatin. Intranuclear cytoplasmic inclusions are almost always present. Hemorrhage, necrosis, and mitotic activity are infrequent findings in medullary carcinomas. A given tumor may be monomorphic showing a predominant cell type or pleomorphic with mixed patterns containing several cell types. The latter is more frequent.
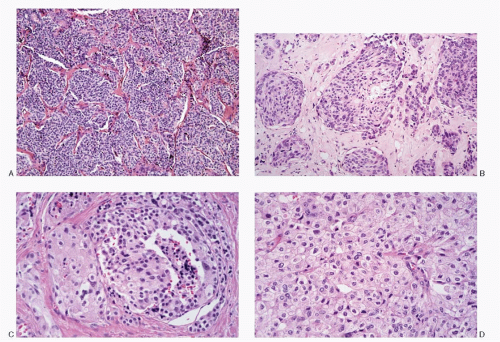 Fig. 8.3: A: Medullary carcinoma showing a lobular growth pattern and is composed of small round cells (H&E). B: Medullary thyroid carcinoma showing lobules of pleomorphic cells of varying size consisting of small to large polygonal and short spindle cells separated by amyloid containing stroma (H&E). C: Medullary thyroid carcinoma. The left half of the field shows tumor composed of large polygonal cells with abundant eosinophilic cytoplasm, while the rest consists of smaller round to cuboidal cells (H&E). D: Medullary carcinoma is composed predominantly of large polygonal cells with abundant eosinophilic cytoplasm bearing a morphologic resemblance to oncocytes (H&E). |
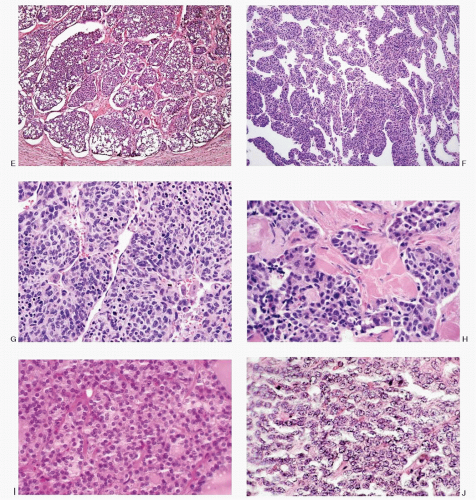 Fig. 8.3: (continued) E: Histologic section of a medullary carcinoma showing a lobular pattern. The lobules vary in size separated by bands of fibrous tissue septae. Also note clear change in the cytoplasm (H&E). F: Medullary carcinoma exhibiting a lobular and a trabecular growth pattern. The trabeculae vary in thickness from slender to broad and are interdigitating (medium power, H&E). G: Higher magnification of (F) showing broad trabeculae consisting of very pleomorphic, round to short spindle-shaped cells (H&E). H: Medullary carcinoma exhibiting nests of small cuboidal cells separated by amyloid (H&E). I: This medullary carcinoma is composed of uniform cuboidal cells forming small nests with a pseudofollicular growth pattern (H&E). J: A solid growth pattern of medullary carcinoma. The cells contain scant to indiscernible cytoplasm (H&E). |
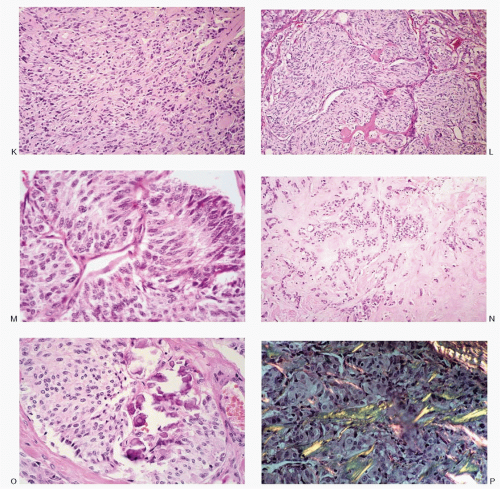 Fig. 8.3: (continued) K: Medullary carcinoma cells are short spindle shaped and separated by stroma (H&E). L: Medullary carcinoma with a spindle cell pattern. The spindle cells are forming large nests separated by fibrous tissue septae (H&E). M: Histologic pattern of this medullary carcinoma with nests of elongated spindle cells resembling a paraganglioma (H&E). N: Medullary carcinoma with abundant amyloid in the stroma. Fine needle aspirates from such areas may be poorly cellular (H&E). O: Medullary carcinoma with stromal fibrosis and calcification (H&E). P: Histologic section of medullary carcinoma showing apple green birefringence of amyloid stained with Congo red (H&E). |
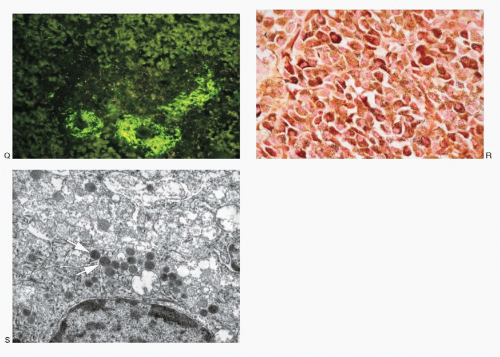 Fig. 8.3: (continued) Q: Bright green fluorescence of amyloid when stained with thioflavin T and viewed under ultraviolet light (H&E). R: Medullary carcinoma demonstrating a strong positive reactivity with calcitonin stain. S: Electron micrograph of medullary carcinoma showing membrane-bound, spherical neurosecretory granules with an electron-dense core (arrow). Uranyl acetate and lead citrate preparation (×42,000). |
TABLE 8.2. IMMUNOPROFILE OF MEDULLARY CARCINOMA | ||||||||||||||||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
|
TABLE 8.3. CYTOPATHOLOGIC FEATURES OF MEDULLARY CARCINOMA | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| ||||||||||||||||||||||||||||||||||||||||||||||||||||||||
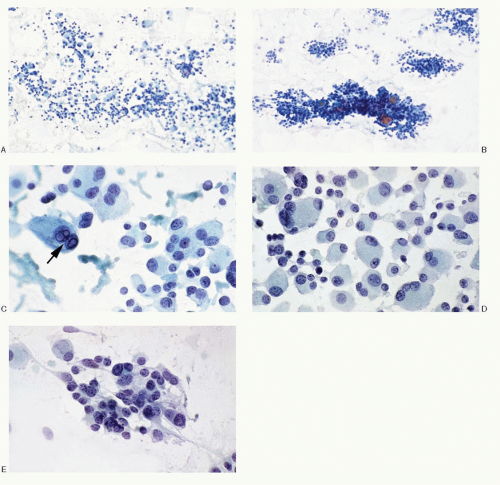 Fig. 8.4: FNA of a Medullary Thyroid Carcinoma. A: Low power showing the characteristic dispersed cell pattern. B: Medium power. Note the syncytial tissue fragments such as seen here are less frequently present. C: Higher magnification showing the discrete, medium-sized to large, pleomorphic, and plasmacytoid neoplastic cells. Binucleation is frequent. Note the intranuclear inclusions (arrow). D: The medullary carcinoma cells are large to giant form with multinucleation. The nuclei have coarse chromatin and exhibit extreme eccentric location. E: Same case, different field, showing a pleomorphic cell pattern with small round cells containing scant cytoplasm, while some cells have cytoplasmic processes. |
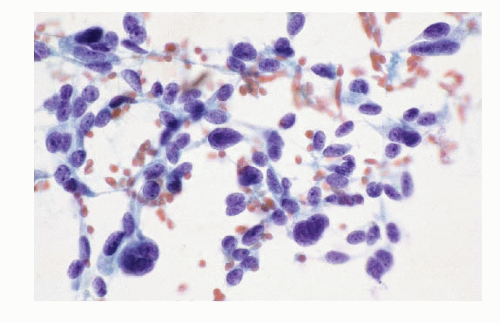 Fig. 8.5: FNA of a Medullary Carcinoma. A pleomorphic cell pattern such as seen here is the hallmark of medullary carcinoma. |
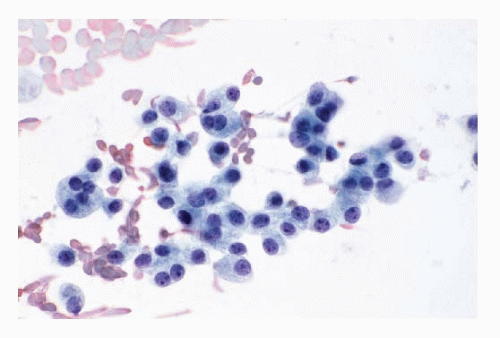 Fig. 8.6: FNA of a Medullary Carcinoma. The cells are very uniform, medium-sized, and plasmacytoid with moderate amount of cytoplasm. These cells strongly resemble either follicular cells or Hürthle cells and may be interpreted as follicular or Hürthle cell neoplasm. |
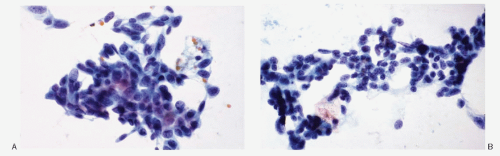 Fig. 8.7: FNA of a Medullary Carcinoma. A: Loosely cohesive medium-sized to large cells consisting of short spindle and cuboidal cells with high N/C ratios and dense nuclear chromatin. B: Another field from the same case showing predominantly small cells with poorly defined cell borders and high N/C ratios. |
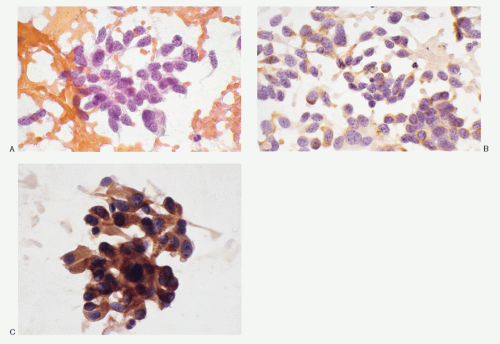 Fig. 8.8: FNA of a Medullary Carcinoma. A: The aspirate shows a pleomorphic cell pattern with coarsely granular nuclear chromatin pattern (salt-pepper) characteristic of a neuroendocrine tumor. Note nucleoli are not appreciated. The cells possess delicate cytoplasmic processes. B: Smear stained for calcitonin showing positive reactivity. C: Different example of medullary carcinoma. Reactivity to calcitonin is usually very strong as demonstrated by these medullary carcinoma cells. |
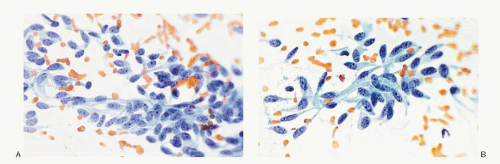 Fig. 8.9: A, B: FNA of a Medullary Carcinoma. A predominant spindle cell pattern with delicate, long, unipolar cytoplasmic processes and eccentric nuclei. Note the characteristic salt-pepper chromatin. |
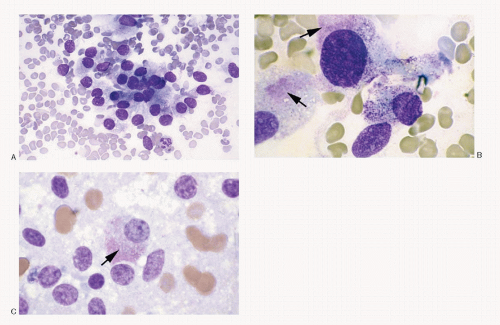 Fig. 8.10: FNA of a Medullary Carcinoma Stained with Romanowsky Stain. A: The cells are loosely cohesive. B, C: These medullary carcinoma cells contain the characteristic azurophilic granules in their cytoplasm (arrows). |
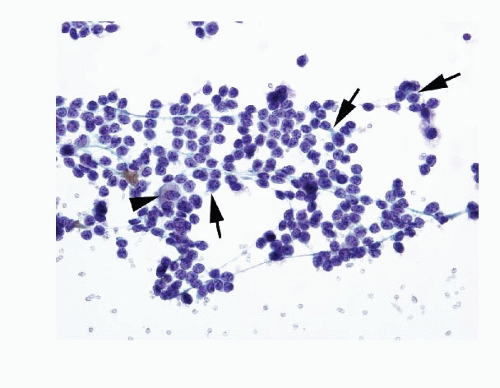 Fig. 8.11: FNA of a Medullary Carcinoma. These medullary carcinoma cells are dispersed, monomorphic, small, round with mostly poorly defined cell borders and scant cytoplasm that is indiscernible to a thin rim of dense cyanophilic (arrows). An occasional cell is large with appreciable cytoplasm. The nuclei are round with coarsely granular chromatin. There is no nuclear molding. With a monomorphic pattern of small round cells, malignant lymphoma must be considered in the differential diagnosis. |
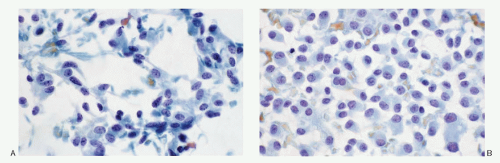 Fig. 8.12: FNA of a Medullary Carcinoma. A: The pleomorphic neoplastic cells are present singly, with many spindle forms possessing cytoplasmic processes. The background contains fluffy acellular material which may represent amyloid. B: Another field from the same case demonstrating plasmacytoid cells with minimal variation in size. |
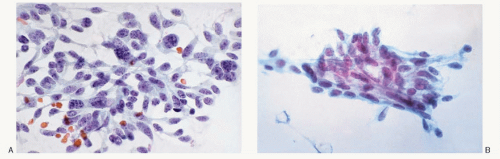 Fig. 8.13: FNA of a Medullary Carcinoma. A: The aspirate is characterized by a pleomorphic cell pattern with predominant spindle cells. Note long cytoplasmic processes, eccentric nuclei, and coarsely granular chromatin. B: Different example of medullary carcinoma with a spindle cell pattern. |
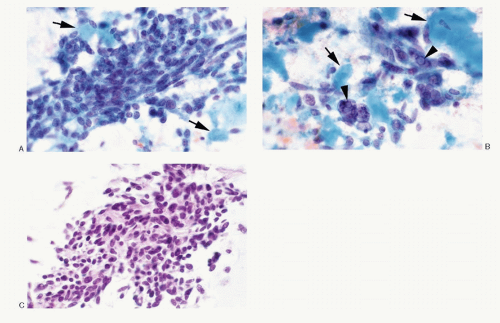 Fig. 8.14: FNA of a Medullary Carcinoma. A: The medullary carcinoma cells are spindle shaped and in fascicles with an admixture of round cells. Note the acellular cyanophilic material in close association with carcinoma cells and probably representing amyloid (arrows). B: A different field showing pleomorphic malignant cells. Note multinucleation and intranuclear inclusions (arrowheads). The background shows abundant dense acellular material that probably represents amyloid (AM). In Papanicolaou-stained smears, amyloid resembles colloid. C: The cell block of the aspirate showing a very pleomorphic, diagnostic cell pattern of medullary carcinoma (H&E).
Stay updated, free articles. Join our Telegram channel
Full access? Get Clinical Tree
 Get Clinical Tree app for offline access
Get Clinical Tree app for offline access

|