Neuroendocrine Tumors of the Skin (Merkel Cell Carcinoma)
Neuroendocrine Tumors of the Skin (Merkel Cell Carcinoma)
Merkel cell carcinoma is a rare and aggressive primary cutaneous neuroendocrine (small cell) carcinoma of the skin arising from the basal epidermis. Toker first described it in 1972 as “trabecular carcinoma” of the skin. The tumor is derived from Merkel cells, which are specialized epithelial cells with neuroendocrine features, more commonly found in the skin with high hair density, in glabrous epithelium of the digits and lips, and in the region of the oral cavity. Fredrich Merkel first identified Merkel cells in 1875 as specific touch-sensitive cells in the skin. Normally, without special stains, Merkel cells cannot be distinguished from the surrounding cells. Ultrastructurally, the Merkel cells demonstrate electrondense, membrane-bound secretory granules and intermediate filament buttons.
Primary neuroendocrine carcinoma of the skin occurs usually in elderly white patients, primarily involving the sun-exposed areas. The incidence is reported to be 0.34/100,000 in men as compared to 0.17/100,000 in women. The majority of the patients are older than 65 years. Nearly half the cases (46%) occur in head and neck, including lip and eyelid, followed by upper extremities 21%, lower extremities 14%, and trunk 7%, with the remaining 7% involving miscellaneous sites.
Clinically, Merkel cell carcinoma presents as a rapidly growing, solitary, purple, dome-shaped papule or plaque on sun-exposed skin, frequently localized in the head and neck region. Merkel cell carcinomas are aggressive tumors with a propensity for local recurrences and metastases to the regional lymph nodes as well as distant sites.
GROSS AND HISTOLOGIC FEATURES
Grossly, Merkel cell carcinomas are confined to the dermis and subcutis and vary in size, ranging from 0.3 to 6 cm with an average of 2 to 3 cm. They appear as gray-white masses.
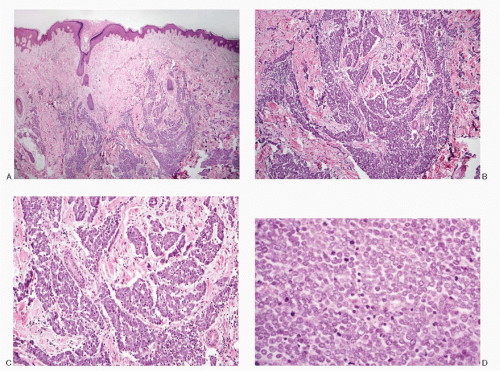
Histologically, Merkel cell carcinomas present two basic growth patterns namely trabecular (Figs. 11.1A-C) and a diffuse, sheet-like growth pattern (Fig. 11.1D), which more closely resembles a malignant lymphoma.
The trabecular pattern consists of cords of tumor cells, two to three cells thick, but the cords can be much wider. The neoplastic cells are round and small with scant rim of amphophilic cytoplasm. The nuclei are round and hyperchromatic with finely granular chromatin and inconspicuous nucleoli. Their N/C ratios are very high. Mitotic activity is usually very brisk. Spindling of the tumor cells can be seen. The Merkel cell carcinoma is usually separated from the epidermis by a zone of dermal collagen (Fig. 11.1A). The tumor is usually restricted to the dermis, but the involvement of subcutaneous fat, fascia, and muscles can be seen. Lymphoplasmacytic infiltrate is often seen surrounding the tumor and within the tumor. Pagetoid growth of the carcinoma cells has been described. The stroma of the tumor is richly vascularized. Areas of coagulative necrosis may produce geographic patterns, and crush artifacts are seen in approximately 50% of the cases. Invasions of the dermal lymphatics and vessels, as well as encrustation of the blood vessels with DNA (“Azzopardi phenomenon/effect”), are other features seen in these tumors. Amyloid deposits have been described. Merkel cell carcinomas may be associated with squamous and basal cell carcinomas.
CYTOPATHOLOGIC FEATURES
The specimens for the cytologic diagnosis of Merkel cell carcinoma usually represent fine needle biopsies of cutaneous nodules or masses and those of metastatic sites such as cervical or mediastinal lymph nodes, salivary glands, skin nodules, and visceral organs. Serous effusion fluid is also utilized to detect metastases.
Fig. 11.1: A: A low-power view of an excised cutaneous nodule showing a dermal neoplasm. Note the band of collagen separating the epidermis and the dermis (H&E). B: At medium power, the neoplasm appears to be very cellular, composed of nests and trabeculae of small neoplastic cells with scant stroma (H&E). C: Higher magnification showing the small, uniform neoplastic cells with high N/C ratios (H&E). D: Histologic section of a different example of Merkel cell carcinoma presenting a solid growth pattern. Note the uniform cells with a brisk mitotic activity (H&E).
The aspirates of Merkel cell carcinomas are usually very cellular, consisting of a large population of monomorphic small, round to cuboidal cells. The neoplastic cells are present as discrete, in loosely cohesive groups or in syncytial tissue fragments without any architectural patterns, closely resembling high-grade neuroendocrine carcinomas (small cell carcinomas) (Table 11.1; Figs. 11.2,11.3,11.4,11.5 and 11.6). Occasionally, pseudorosettes may be present. The neoplastic cells are also seen clustering around the blood vessels. Their cell borders are poorly defined, and the cytoplasm is indiscernible to scant. The nuclei are round to oval with high N/C ratios. Their chromatin is granular; nuclear molding and stretch artifacts may be noted. The nuclear membranes are smooth to irregular and occasionally highly convoluted. Mitoses are frequent as is individual cell necrosis. Merkel cell carcinoma cells have scant cytoplasm, but occasionally it appears pale-pink, homogeneous with well-circumscribed round-to-oval buttons of dense cytoplasm in perinuclear locations. These buttons are described as either attached to the nucleus, lying in the indentation of the nucleus, or detached, lying free outside the nucleus. Ultrastructurally, these correspond to the distinct whorls of intermediate filaments (Fig. 11.7D).
TABLE 11.1. CYTOLOGIC FEATURES OF MERKEL CELL (CUTANEOUS NEUROENDOCRINE) CARCINOMA
Cellularity
Highly cellular
Presentation
Dissociated pattern common, cells mostly isolated; also in groups and in syncytial tissue fragments
Cells
Monomorphic, small, round, 10-16 µm in largest dimension; poorly defined cell borders; high N/C ratios
Nucleus
Round to oval; smooth nuclear membrane; convoluted shapes have been described; salt-pepper chromatin; nucleolus +/-; mitoses frequent; nuclear molding +/-; karyorrhexis +/-; stretch artifacts +/-
Cytoplasm
Indiscernible to scant
Background
Necrosis +/-; stripped nuclei
Immunoprofile
Positive reactivity to neuroendocrine markers; neurofilament protein; low molecular weight cytokeratin and CK20; negative reactivity to CK7; TTF-1; S100 protein, high molecular weight keratin, and leukocyte common antigen (LCA)
Ultrastructure
Electron-dense, membrane-bound secretory granules; paranuclear whorls or buttons of intermediate filaments
Merkel cell carcinoma cells react positively to several neuroendocrine markers such as chromogranin, synaptophysin, and neuron-specific enolase. The cells are reactive to low molecular weight keratin, cytokeratin 20 (CK20), and neurofilament protein. Merkel cell carcinoma cells are nonreactive to high molecular weight keratin and thyroid transcription factor-1 (TTF-1). The positive reactivity to CK20 and the negative reactivity to TTF-1 are important features that differentiate pulmonary small cell carcinomas from Merkel cell carcinoma.
ULTRASTRUCTURE
Ultrastructurally, Merkel cell carcinoma cells invariably demonstrate membrane-bound, dense-core secretory granules, 80 to 300 nm in diameter. In many cases, the granules demonstrate a clear zone surrounding the dense-core granules. Another important feature is the presence of perinuclear or juxtanuclear whorls of intermediate filaments, an important feature that differentiates Merkel cell carcinoma from other neuroendocrine tumors (Fig. 11.7D).
DIAGNOSTIC ACCURACY AND DIFFERENTIAL DIAGNOSES
The cytomorphology of Merkel cell carcinoma is characteristic enough to suggest the diagnosis when the primary site is head and neck or sun-exposed area and is supported by immunostains. However, the diagnostic problems are encountered with Merkel cell carcinomas at the metastatic sites.
The cytological differential diagnoses of Merkel cell carcinoma include neoplasms that are composed of small cells and are site specific. Primary Merkel cell carcinoma presents an overlapping pattern with cutaneous lesions such as poorly differentiated squamous carcinoma, basaloid squamous carcinoma, metastatic neuroendocrine carcinomas to the skin, for example, small cell carcinomas and metastatic carcinoid tumors, and malignant non-Hodgkin lymphoma/leukemia. Merkel cell carcinoma often metastasizes to the salivary glands, particularly the parotid gland, and must be differentiated from neoplasms composed of small cells such as primary or metastatic small cell neuroendocrine carcinoma, adenoid cystic carcinoma, malignant lymphoma/leukemia, metastatic poorly differentiated squamous and adenocarcinomas, and malignant melanoma. The same holds true with aspirates of metastatic Merkel cell carcinoma at various body sites. History of Merkel cell carcinoma is critical. The differentiating features of diagnostic entities are listed in Table 11.2 and illustrated in Figures 11.8,11.9,11.10,11.11,11.12 and 11.13. Ancillary tests are required for accurate typing of the neoplasm.
Only gold members can continue reading. Log In or Register to continue