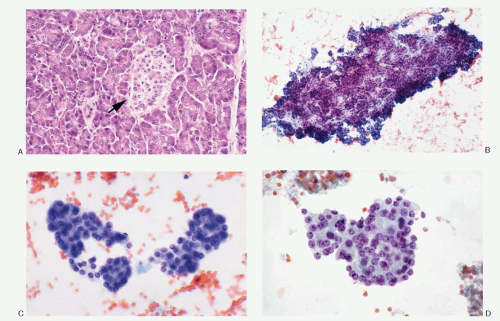
 Fig. 5.1: Normal Histology and Cytology of the Pancreas (Exocrine and Endocrine). A: Histologic section of the pancreas showing acinar tissue formed by large triangular cells containing abundant eosinophilic granular cytoplasm, basally located round nuclei. An islet of Langerhans is seen in the center of the field (arrow). The component cells (neuroendocrine) of the islet are smaller, with scant, pale eosinophilic cytoplasm, uniform round nuclei, and high N/C ratios (H&E). B: Fine needle aspiration (FNA) biopsy specimen showing normal pancreatic acinar tissue (low power). C, D: Higher magnification depicting the cytomorphology of the acinar cells. Normal islet cells usually not seen in the aspirated samples. |
and jaundice. In case of functioning tumors, the presenting signs depend on the effects of hormone secreted by the tumor.
TABLE 5.1. PANCREATIC NEUROENDOCRINE TUMORS (NETS) IN HEREDITARY SYNDROMES | ||||||||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
|
considerably within the same tumor. Although the architectural pattern suggests the endocrine nature, there is no reliable relationship between architectural patterns and the cell type, hormone production, or biologic behavior. The tumor cells are generally uniform in size and shape. They may be round, polygonal, or elongated. The cell borders are usually well-defined. The cytoplasm is eosinophilic or clear. The nuclei are uniform, and the nucleoli range from inconspicuous to prominent. The salt-pepper chromatin is characteristic but not universally present. Pleomorphic large cells may be scattered throughout the tumor. Mitoses are generally rare. The cytoplasm is usually scant but can be appreciable and eosinophilic in oncocytic variants. PETs are richly vascular with a prominent capillary network. Hyalinization of the tumor stroma is common and may be extensive. Amyloid is sometimes present, especially in insulinomas.
 Fig. 5.2: Gross Photograph of Pancreatic Neuroendocrine Tumor. Well-defined, large tumor with a bulging cut surface. |
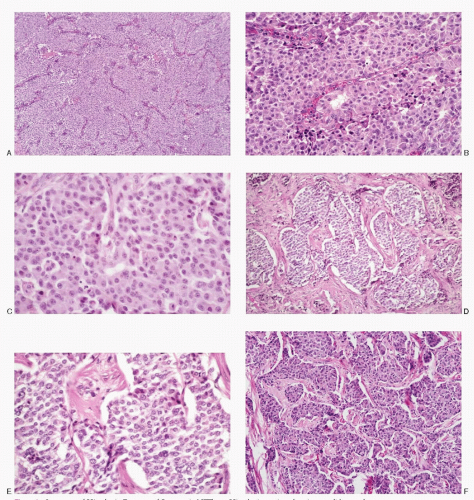 Fig. 5.3: Spectrum of Histologic Features of Pancreatic NETs. A: Histologic section showing a solid growth pattern (low power, H&E). B: Medium-sized cells with modest eosinophilic cytoplasm, central to eccentric uniform nuclei (H&E). C: A closer view of a PET showing round to cuboidal cells with moderate amounts of eosinophilic cytoplasm. The nuclear chromatin is granular (H&E). D: Broad trabeculae separated by abundant stroma (H&E). E: Higher magnification of D showing uniform cells with insignificant cytoplasm (H&E). F: Neuroendocrine tumor with broad trabeculae and insulae consisting of moderately pleomorphic nuclei. The cells are larger with appreciable eosinophilic cytoplasm. |
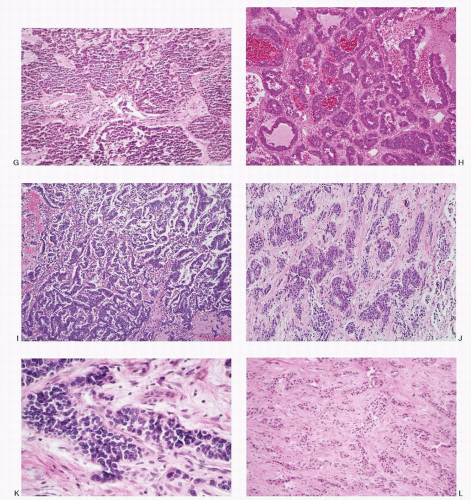 Fig. 5.3: (continued) G: Neuroendocrine carcinoma depicting an insular pattern consisting of small uniform cells (H&E). H: Neuroendocrine tumor presenting an acinar and a pseudopapillary pattern (H&E). I: This neuroendocrine tumor consists of delicate cords with an anastomosing pattern (H&E). J: Fibrous tissue strands separating islands of neoplastic cells (H&E). K: Higher magnification showing smaller neoplastic cells with hyperchromatic nuclei (H&E). L: This pancreatic neuroendocrine tumor shows cords and nests of uniform tumor cells diffusely infiltrating the extensive fibrous stroma (H&E). |
(Figs. 5.7, 5.9,5.10,5.11 and 5.12, and 5.14) or a pleomorphic pattern (Figs. 5.4,5.5 and 5.6, 5.8, 5.9, and 5.13). The nuclei are round to oval; nuclear membranes are smooth and crisp. The chromatin is characteristic of the neuroendocrine family of tumors, being uniformly and coarsely granular presenting a salt-pepper pattern. Nucleoli are not consistently present. The nuclei tend to be uniform but may be variable in size. The cytoplasm ranges from scant to moderate, pale to dense, and is eosinophilic in oncocytic variant. Capillary network may be prominent in the background and neoplastic cells may be seen in perivascular location. Mitotic activity or necrosis is usually not present but can be seen in widely invasive NETs (Fig. 5.5). The cell block preparations can be extremely useful in the diagnostic evaluation since they allow ancillary testings.
TABLE 5.2. TYPES OF SPECIMENS FOR CYTOPATHOLOGIC DIAGNOSIS OF PANCREATIC ENDOCRINE TUMORS | |
|---|---|
|
TABLE 5.3. CYTOPATHOLOGIC FEATURES OF PANCREATIC NEUROENDOCRINE TUMORS | ||||||||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
|
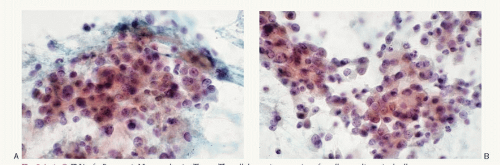 Fig. 5.4: A-C: FNA of a Pancreatic Neuroendocrine Tumor. The cellular aspirate consists of small to medium-sized cells in loosely cohesive groups and syncytial tissue fragments. The cells have poorly defined cell borders, scant cytoplasm, and pleomorphic nuclei containing coarsely granular chromatin. Some contain nucleoli. |
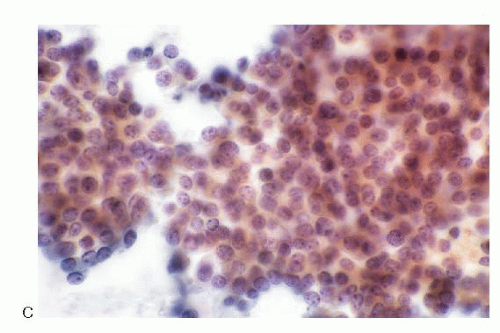 Fig. 5.4: (continued) |
 Fig. 5.5: FNA of Pancreatic Neuroendocrine Tumor. A: This aspirate consists of discrete cells that are uniform, small with poorly defined cell borders, high N/C ratios. The nuclear chromatin is typical salt-pepper type. B: This field shows an area of necrosis (arrow). |
 Fig. 5.6: A, B: FNA of a Pancreatic Neuroendocrine Tumor. The aspirate reveals dissociated cell pattern. The neoplastic cells are pleomorphic in size and shape. The nuclear chromatin is salt-pepper type. |
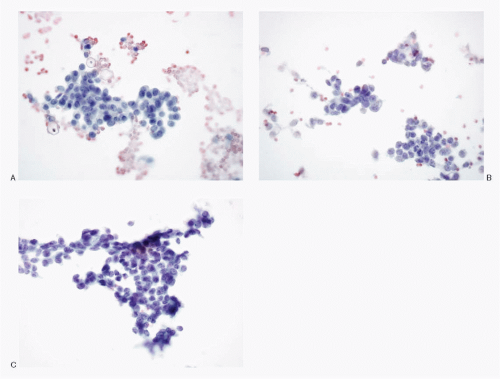 Fig. 5.7: A-C: FNA of a Pancreatic Neuroendocrine Tumor. The cellular aspirate shows syncytial tissue fragments of uniform small cells with bland chromatin pattern. |
 Fig. 5.8: FNA of a Pancreatic Neuroendocrine Tumor. A: This image shows a dispersed pattern of plasmacytoid cells with occasional giant forms. B: Same case stained by H&E. (Courtesy of Dr. Mithra Baliga, University of Mississippi, Jackson, Mississippi.)
Stay updated, free articles. Join our Telegram channel
Full access? Get Clinical Tree
 Get Clinical Tree app for offline access
Get Clinical Tree app for offline access

|