preparations are extremely crowded and overlapped and their morphology may not be well visualized.
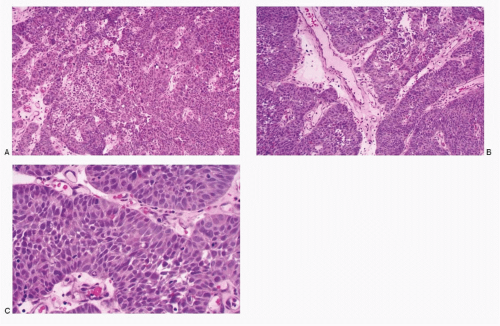 Fig. 12.1: Histologic Sections of Poorly Differentiated Neuroendocrine (Small Cell) Carcinoma of the Uterine Cervix. A, B: Mediumpower view showing a solid and trabecular growth pattern (H&E). C: Higher magnification showing peripheral palisading of nuclei. The cells are short spindle shaped with high N/C ratios (H&E). |
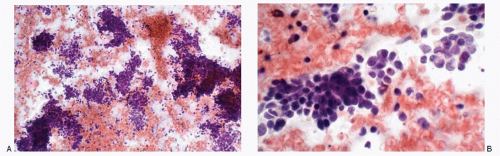 Fig. 12.2: Conventional Cervical Smear from the Same Case as Figure 12.1. A: Medium-power view, showing a large population of malignant cells in varying-sized syncytial tissue fragments. B: Higher magnification demonstrating the large population of small malignant cells, with mildly pleomorphic nuclei containing compact chromatin. Nucleoli are not seen. Nuclear molding can be appreciated. The cell borders are poorly defined, and the cytoplasm is indistinct with high N/C ratios. |
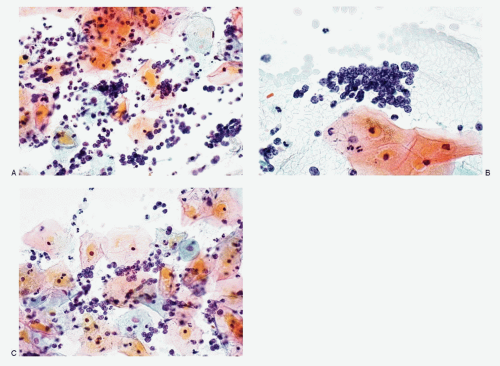 Fig. 12.3: A-C: Another example of histologically proven small cell neuroendocrine carcinoma of the uterine cervix. The malignant cells are discrete and loosely cohesive, small with poorly defined cell borders, scant, indiscernible cytoplasm, and high N/C ratios. Note single cells are difficult to type as malignant. Note the classic salt-pepper chromatin in B (conventional smear). |
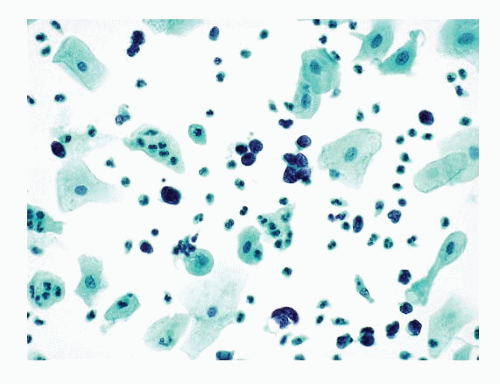 Fig. 12.4: Liquid-Based Preparation of a Cervical Smear, Depicting Small Cell Carcinoma Cells. Note the number of malignant cells is very small and they are present isolated or in small groups. They resemble lymphoid cells as no features suggestive of small cell carcinoma are readily appreciated. (Courtesy of Ms. Karen Atkinson, MPA, CT (ASCP), CMIAC, Director of Education and Training, and Mr. Tim Collins, BS, CT (ASCP), Senior Scientist, Research and Development, BD Diagnostics-Women’s Health and Cancer, Burlington, North Carolina.) |
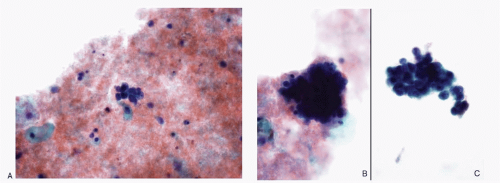 Fig. 12.5: A-C: Liquid-based preparation of a cervical smear, depicting small cell carcinoma cells from a case of histologically confirmed small cell neuroendocrine carcinoma. Note that these cells are in tight three-dimensional groups and their cytomorphology is not readily apparent. Cervical biopsy revealed a small cell neuroendocrine carcinoma. |
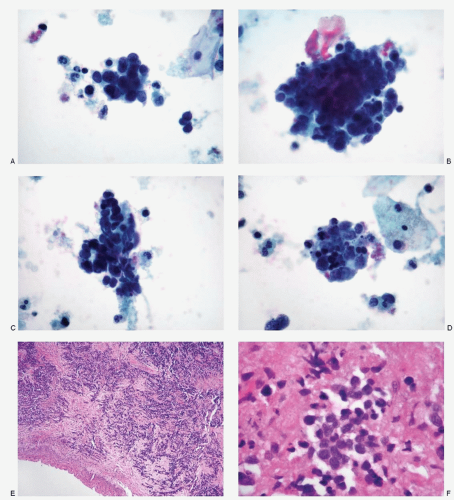 Fig. 12.6: A 38-year-old woman with a history of multiple abnormal pap smears complained of right lower quadrant pain. Pelvic examination revealed a large cervical mass. A pap smear was obtained and multiple cervical biopsies were done. A-D: Liquid-based preparation of a cervical smear showing syncytial tissue fragments of small cells with poorly defined cell borders, very high N/C ratios, and indistinct cytoplasm. The nuclear chromatin is compact and deep staining. A few discrete cells are present in the background. The smear was interpreted as high-grade squamous intraepithelial lesion. The cervical biopsies revealed a widely invasive small cell carcinoma. E: This low-power view of the cervical biopsy shows a small cell carcinoma in subepithelial location and diffusely infiltrating the cervical stroma (H&E). F: Higher magnification highlighting the small cell carcinoma. (Courtesy of Dr. Mithra Baliga, University of Mississippi, Jackson, Mississippi.) |
TABLE 12.1. DIFFERENTIAL DIAGNOSES OF SMALL CELL CARCINOMA OF THE UTERINE CERVIX | ||||||||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
|
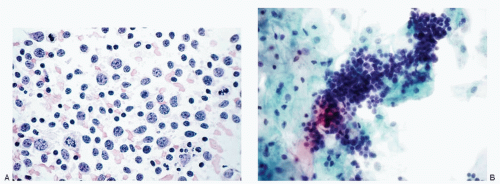 Fig. 12.7: A: Conventional cervical smear showing a polymorphic lymphoid cell population consistent with lymphofollicular cervicitis. B: Liquid-based preparation showing a tight aggregate of lymphoid cells that can be mistaken for a small cell carcinoma. |
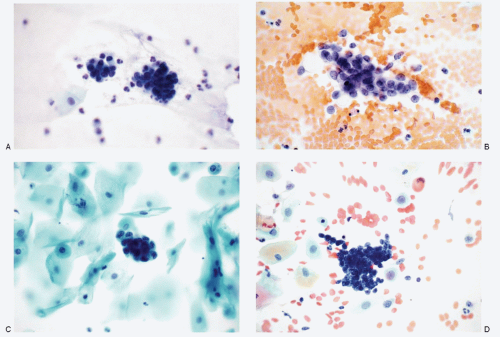 Fig. 12.8: Endometrial Cells and Endometrial Adenocarcinoma. A, B: These two different conventional smears contain well-preserved endometrial cells, which morphologically resemble small cell carcinoma cells. C: Liquid-based preparation showing endometrial cells. D: Conventional cervical smear showing cells of well-differentiated endometrial adenocarcinoma.
Stay updated, free articles. Join our Telegram channel
Full access? Get Clinical Tree
 Get Clinical Tree app for offline access
Get Clinical Tree app for offline access

|