Neuroendocrine Carcinomas of the Thymus
Key Facts
Terminology
Synonyms: Carcinoid tumor, atypical carcinoid, small cell carcinoma
Malignant neoplasms that range from low- to high-grade malignancies
Clinical Issues
Incidence
Thymic neuroendocrine carcinomas represent approximately 5% of all mediastinal tumors
Can occur at any age
Symptoms
Paraneoplastic syndromes
Multiple endocrine neoplasia, type II (MEN-II)
Cushing syndrome
Prognosis depends on grade and surgical stage of neoplasm at time of diagnosis
WDNECa: 5-year survival approximately 50%
MDNECa: 5-year survival approximately 25%
PDNECa: 5-year survival 0%
Treatment
Complete surgical resection
Surgical resection followed by chemotherapy in higher grade tumors
Top Differential Diagnoses
Paraganglioma
Ectopic parathyroid tumor
Thymic carcinoma
Diagnostic Checklist
Nesting growth pattern
Mitotic activity
Presence of necrosis
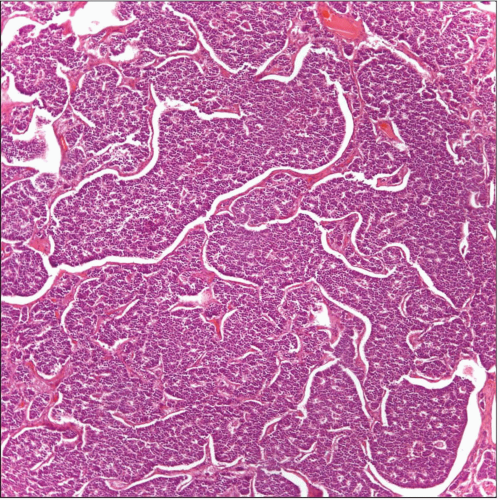 Well-differentiated neuroendocrine carcinoma (carcinoid tumor) shows a cellular proliferation arranged in cords and nests. |
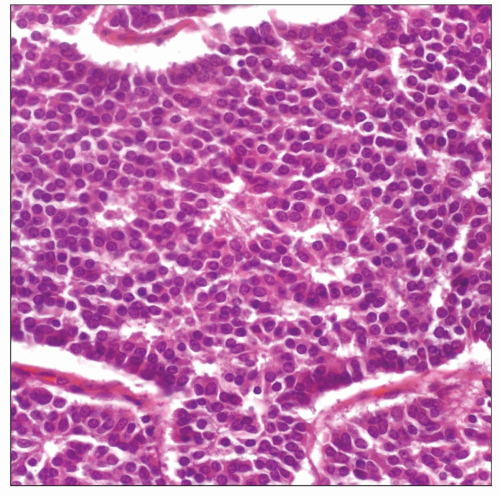 High-power magnification of a well-differentiated neuroendocrine carcinoma (carcinoid tumor) shows a homogeneous cellular proliferation without nuclear atypia or mitotic activity. |
TERMINOLOGY
Abbreviations
Well-differentiated neuroendocrine carcinoma (WDNECa)
Moderately differentiated neuroendocrine carcinoma (MDNECa)
Poorly differentiated neuroendocrine carcinoma (PDNECa)
Synonyms
Carcinoid tumor, atypical carcinoid, small cell carcinoma
Definitions
Malignant neuroendocrine neoplasms that range from low- to high-grade malignancies
ETIOLOGY/PATHOGENESIS
Etiology
Probably originating from Kulchitsky cells
CLINICAL ISSUES
Epidemiology
Incidence
Thymic neuroendocrine carcinomas represent approximately 5% of all mediastinal tumors
Age
Neuroendocrine carcinomas can occur in any age group
Gender
No specific gender predilection for thymic neuroendocrine carcinomas
Site
Anterior mediastinum
Presentation
Chest pain
Cough
Dyspnea
Cushing syndrome
Multiple endocrine neoplasia, type II (MEN-II)
Proximal myopathy
Polyarthropathy
Peripheral neuropathy
Incomplete Sipple syndrome
ADH secretion
Eaton-Lambert syndrome
Hypertrophic osteoarthropathy
ACTH secretion
Paraneoplastic syndromes
Treatment
Complete surgical resection
Depending on grade of tumor
Surgical resection followed by chemotherapy
In poorly differentiated tumors (small cell carcinoma): Chemotherapy
Prognosis
Depends on grade and surgical stage of neoplasm at time of diagnosis
WDNECa: 5-year survival approximately 50%
MDNECa: 5-year survival approximately 25%
PDNECa: 5-year survival 0%
MACROSCOPIC FEATURES
General Features
Tan to brown color
Soft consistency
Well-defined but not encapsulated tumor
Areas of hemorrhage &/or necrosis may be present
Minority of cases will present with cystic changes
Sections to Be Submitted
Important to document transitional areas of tumor and normal thymus
Important to document presence of necrosis &/or hemorrhage
Size
Variable size from a few cm to > 10 cm in diameter
MICROSCOPIC PATHOLOGY
Histologic Features
Nesting growth pattern
Spindle cell growth pattern
Oncocytic growth pattern
Pigmented
Cystic
Angiomatoid growth pattern
DIFFERENTIAL DIAGNOSIS
Paraganglioma
Paraganglioma and neuroendocrine carcinomas may share similar immunophenotype in terms of neuroendocrine markers
Usually negative for keratin markers
May show presence of prominent nuclear atypia, but mitotic activity is rare
Ectopic Parathyroid Tumor
May also share similar immunophenotype
May show the presence of chief and oncocytic cells
Generally shows positive staining for PTH
Shows positive staining for PAS
Thymoma
May show areas that mimic histologically a neuroendocrine tumor
Generally negative for neuroendocrine markers
Thymic Carcinoma
Usually negative for neuroendocrine markers
Histology of thymic carcinoma is different from “neuroendocrine pattern” seen in neuroendocrine tumors
Metastatic Neuroendocrine Carcinoma
Clinical history is important tool in arriving at specific site of origin
Use of immunohistochemical studies in some cases may provide a clue for site of origin
DIAGNOSTIC CHECKLIST
Clinically Relevant Pathologic Features
Nuclear features
Mitotic rate
Invasive pattern
Pathologic Interpretation Pearls
Nesting growth pattern
Mitotic activity
Presence of necrosis
SELECTED REFERENCES
1. Moran CA et al: Cystic well-differentiated neuroendocrine carcinoma (carcinoid tumor): a clinicopathologic and immunohistochemical study of two cases. Am J Clin Pathol. 126(3):377-80, 2006
2. Moran CA: Primary neuroendocrine carcinomas of the mediastinum: review of current criteria for histopathologic diagnosis and classification. Semin Diagn Pathol. 22(3):223-9, 2005
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


