Aperson who forgets his identity and turns out to be the long-lost heir to a fortune is the stuff of novels and movies. In the real world, amnesia (loss of memory) rarely has a romantic or exciting outcome. Two groups of disorders, the neurocognitive disorders and the dissociative disorders, are characterized by deficits in memory function, as well as personality changes and unusual behavior. Although they may have similar presentations, the etiology of these two groups of disorders is quite different. In the neurocognitive disorders, symptoms result from anatomic or metabolic abnormalities in the brain itself. In the dissociative disorders, symptoms are psychological, often associated with emotional stress that has occurred in the individual’s recent or remote past.
• NEUROCOGNITIVE DISORDERS
Neurocognitive disorders involve problems with memory, as well as difficulty with orientation to person, place, and time (orientation times three), level of consciousness, and other neurocognitive or “thinking” functions. These symptoms are caused by abnormalities in neural chemistry, structure, or physiology originating in the brain or secondary to systemic illness. Patients with neurocognitive disorders may have psychiatric symptoms, such as mood changes, anxiety, irritability, paranoia, and psychosis. These symptoms, while secondary to the neurocognitive losses, can lead to misdiagnosis. The American folk singer Woody Guthrie, who died of Huntington’s disease in 1967, was incorrectly diagnosed early in the illness with “schizophrenia, paranoid type.”
Because all psychiatric symptoms are mediated by the brain, it is theoretically difficult to separate organic from nonorganic disorders. Therefore, neurocognitive disorders are no longer termed organic mental disorders. The neurocognitive disorders in the Diagnostic and Statistical Manual of MentalDisorders, Fifth Edition (DSM-5) are delirium, and major and mild neurocognitive disorder (dementia). Amnestic disorder is classified in the DSM-5 as major or mild neurocognitive disorder due to a medical condition.
Differential diagnosis of the neurocognitive disorders
Many patients with neurocognitive disorders are elderly. Because normal aging is associated with minor neurocognitive changes, such as reduction in the ability to learn new things quickly and a general slowing of mental processes, it may be necessary for a physician to make the distinction between normal aging and a neurocognitive disorder in an individual patient. One important distinction between these two entities is that, in contrast to patients with neurocognitive disorders whose functioning is quite impaired, normally aging patients are able to care for themselves and carry on a normal life.
Depressed patients, particularly when elderly, often show difficulties in concentration and decreased speed of mental processes. This presentation of depression is often called pseudodementia because it mimics neurocognitive impairment (see Chapter 4) (Table 18-1).
Delirium
Delirium is a syndrome of neurocognitive impairment that results from central nervous system dysfunction; it is characterized by clouding of consciousness. Commonly, delirious patients are oriented to person but are not fully attentive, and they are not oriented to time or place. The patient also often appears to be hyperactive or hypoactive and seems anxious and confused. Sleep disturbances and autonomic dysfunction are common in delirium.
Delirium usually presents in the course of an acute medical illness. It is the most common psychiatric syndrome seen in hospitalized patients, particularly those in surgical and coronary intensive care units, and in elderly nursing home patients with illnesses such as systemic infections (e.g., urosepsis). The disorder is more common also in children and in patients with preexisting brain damage or a history of psychiatric illness.
Some of the most common causes of delirium are diseases of the central nervous system, such as meningitis and encephalitis; systemic illnesses originating in the liver, kidney, heart, or lungs; and substance abuse and withdrawal, particularly involving the sedative drugs, such as alcohol. Other causes of delirium include opportunistic infection of the brain resulting from HIV infection, acute electrolyte changes, fever, postoperative states, and medications such as anticholinergics (see Table 25-4).
table 18.1 COMPARISON OF DEPRESSION, DELIRIUM, AND DEMENTIA
DEPRESSION
DELIRIUM
DEMENTIA
Hallmark
Sad mood
Impaired consciousness
Loss of intellectual ability
Patient example
A 67-year-old retired former banker cannot remember to pay his bills. He has also lost more than 10 lb (4.5 kg) and wakes 2 hours before his alarm. His symptoms started after he gave up his driver’s license
After an acute myocardial infarction, a 67-year-old former policeman with no earlier history of psychiatric illness seems confused and agitated and reports seeing strange animals in his hospital room
A 67-year-old retired legal secretary is alert but has shown increasing memory problems over the past few years. She neither knows what day it is nor can she identify her daughter who is sitting next to her
Consciousness
Not impaired
Impaired or clouded
Not impaired
Speed of development
Slow
Fast
Slow
Level of arousal
Normal
Stupor or agitation
Normal
Psychotic symptoms
Uncommon
Common (particularly visual hallucinations)
Uncommon
Autonomic dysfunction
Little
Severe
Little
Electroencephalogram
Usually normal
Fast wave activity or generalized slowing
Usually normal
Diurnal variability
Worse in the morning
Worse at night (i.e., “sun downing”)
Worse at night
Reversibility
Usually reversible with antidepressant treatment or electroconvulsive therapy
Usually reversible if the underlying medical cause is effectively managed
Rarely reversible
Delirium can progress to dementia or death if left untreated. However, if a delirious patient is identified (using an instrument such as the Folstein Mini-Mental State Examination; see Table 6-6) and the underlying medical cause treated effectively, the prognosis is good. Psychological management includes providing patients with ongoing orienting information about where they are and who their caregivers are as well as the current location, date, and time of day.
Dementia
Dementia is characterized by gradual loss of memory and intellectual abilities without impairment of consciousness. It most commonly occurs in the elderly; more than 20% of individuals 80 years of age and older exhibit some form of this disorder. Dementia of the Alzheimer’s type (hereinafter Alzheimer’s disease), makes up one-half to two-thirds of cases of dementia. Other causes of dementia include vascular dementia and Lewy body dementia, as well as dementias caused by HIV and other infectious processes (e.g., Creutzfeldt-Jakob disease). Each of these disorders can receive the DSM-5 classification of major or mild neurocognitive disorder with a specifier, e.g., due to Alzheimer’s disease.
Alzheimer’s disease While the etiology of Alzheimer’s disease is unknown, factors that have been implicated include micro- and macroscopic neuroanatomical changes (e.g., accumulation of β-amyloid plaques at the ends of degenerating neurons [Helmuth, 2002]) and genetic components (see Table 5-2) (e.g., possession of at least one copy of the apolipoprotein E4 gene). Other factors include neurotransmitter alterations, such as reduction in brain levels of choline acetyltransferase that is needed to synthesize acetylcholine, and overstimulation of the N-methyl-D-aspartate (NMDA) receptor by glutamate (Reisberg et al., 2003) (Table 18-2).
Alzheimer’s disease has a slow, insidious onset and a progressive, irreversible, downhill course. Cognitive function deteriorates; however, patients usually have a normal level of consciousness and retain motor ability until the later stage of the illness. Neuroanatomically, the illness typically progresses from temporal to frontal and parietal lobes (Fig. 18-1), sparing the occipital lobes and primary motor and sensory strips. A patient with Alzheimer’s disease typically first shows memory loss; then has difficulty finding the right words; then becomes unable to copy a simple drawing, often with intact ambulatory function.
Frontal involvement is associated with the development of emotional symptoms such as anger, depression, and anxiety; difficulty controlling impulses; and lack of judgment. Late-stage symptoms include confusion, psychosis, apathy, and agitation that progress to coma and death, usually within 8 to 10 years of diagnosis.
Management of patients with Alzheimer’s disease The most effective initial intervention in Alzheimer’s disease involves providing a structured environment for the patient, including visual orienting cues. Such cues include labels over the doors of rooms identifying their function; daily posting of the day of the week, date, and year; and daily written activity schedules. Practical safety measures, such as disconnecting the stove, are also advisable. Providing a nutritious diet, exercise, and recreational therapy for the patient, as well as psychotherapy and support groups for family caretakers, is crucial in managing the Alzheimer’s patient. Despite such interventions, increasing levels of dementia and disability ultimately lead to nursing home placement for most patients.
table 18.2 PATHOPHYSIOLOGY OF ALZHEIMER’S DISEASE
Gross Neuroanatomy
Enlarged ventricles
Diffuse atrophy
Flattened cortical sulci
Microscopic Neuroanatomy
Amyloid plaques
Neurofibrillary tangles (seen also in Down’s syndrome and, to a lesser extent, in normal aging) in cortex, hippocampus, locus ceruleus, and substantia nigra
Loss of cholinergic neurons in the basal forebrain
Neuronal loss and degeneration in the hippocampus and cortex
Neurophysiology
Reduction in brain levels of choline acetyltransferase, which is needed to synthesize acetylcholine
Abnormal processing of amyloid precursor protein
Decreased membrane fluidity caused by abnormal regulation of membrane phospholipid metabolism
Abnormalities of chromosome 21 (site of gene for amyloid precursor protein)
Abnormalities of chromosomes 1 and 14 (sites of Presenilin 2 and Presenilin 1 genes)
Possession of at least one copy of the apolipoprotein E4 gene (apoE4) on chromosome 19 (particularly in women)
Having a close relative with Alzheimer’s disease
Female gender
Neurotransmitter Relationships
Hypoactivity of acetylcholine and norepinephrine
Overstimulation of the NMDA receptor by glutamate
Hypoactivity of somatostatin, vasoactive intestinal peptide, and corticotropin
Although there is currently no agent that can restore neurocognitive function, pharmacotherapy has a role in the treatment of patients with Alzheimer’s disease. Acetylcholinesterase inhibitors (see also Chapter 19) prevent the breakdown of acetylcholine, improve neurocognitive function transiently, and slow the progression of disease in about 25% of patients. Donepezil (Aricept) and newer cholinesterase inhibitors such as rivastigmine (Exelon) and galantamine (Razadyne) have fewer adverse hepatic and gastrointestinal effects than an older agent, tacrine (Cognex). In the last decade, an NMDA antagonist, memantine (Namenda), was shown to be effective in slowing clinical deterioration in patients with moderate to severe Alzheimer’s disease. The action of memantine is to modulate the NMDA receptor calcium channel thus protecting the neurons from excitotoxicity caused by the influx of excessive glutamate and calcium which are released by other impaired neurons (see Chapter 5).
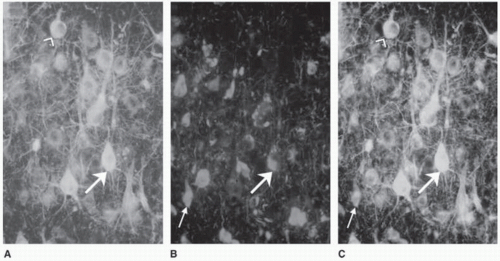
FIGURE 18-1. Neurons in a human brain with Alzheimer disease. Normal neurons contain neurofilaments but no neurofibrillary tangles. (A) Brain tissue stained by a method that makes neuronal neurofilaments fluoresce showing viable neurons. (B) The same region of the brain as shown in part A stained to show the presence of tau within neurofibrillary tangles. (C) Superimposition of the images in parts A and B. The neuron indicated by the arrowhead (ˆ) contains neurofilaments but no tangles and is thus healthy. The neuron indicated by the large arrow has neurofilaments but has also started to show accumulation of tau and thus is diseased. The neuron indicated by the small arrow is dead because it contains no neurofilaments. The remaining tangle is the tombstone of a neuron killed by Alzheimer disease. (Reprinted with permission from Bear MF, Connors BW, Paradiso MA. Neuroscience: Exploring the Brain (3rd ed.). Philadelphia: Lippincott Williams & Wilkins; 2006.)
Agents that decrease the amount of β-amyloid in the brain by promoting immune system attack on β-amyloid plaques and decreasing cholesterol that fosters β-amyloid production are in development (Helmuth, 2002; Vega et al., 2003). Antianxiety agents, antidepressants, and antipsychotics (see Chapter 19) also can be helpful for treating the associated emotional symptoms of Alzheimer’s disease (Meyers and Jeste, 2010).
Vascular dementia Vascular dementia makes up about 15% to 30% of dementias. Vascular dementia is caused by multiple, small cerebral infarctions resulting from atherosclerosis, valvular heart disease, or arrhythmias (Fig. 18-2). Between 30% and 40% of patients with Alzheimer’s disease have a vascular component to their symptoms. In contrast to Alzheimer’s dementia, vascular dementias are characterized by the following:
Sudden rather than gradual onset of neurocognitive dysfunction
Stepwise, abrupt loss of some function with each infarct rather than steady deterioration (e.g., an elderly patient whose mental functioning has been normal suddenly cannot remember what to do with the phone when it rings or how to turn on the microwave)
Better preservation of the patient’s personality characteristics
Higher risk for men than for women
Increased likelihood of focal neurologic signs
To manage vascular dementias, it is important to reduce the likelihood of new infarcts by using anticlotting agents as well as by treating medical risk factors associated with cerebrovascular disease, such as hypertension and cardiac arrhythmias. In addition, the need to reduce behavioral risk factors, such as excessive body weight, smoking, and alcohol abuse, must be addressed.
Other dementias Lewy body dementia, once viewed as a variant of Alzheimer’s disease, appears to be a distinct clinical disorder. It is characterized by a gradually progressive loss of neurocognitive abilities as well as hallucinations, often visual, and the motor characteristics of Parkinson’s disease. Neuroanatomical findings include Lewy inclusion bodies (round, eosinophilic inclusions consisting
Only gold members can continue reading. Log In or Register to continue