The anterior part of the pituitary gland, also referred to as adenohypophysis, is one of the two organs in the dispersed neuroendocrine system that are entirely composed of neuroendocrine cells. Pituitary neoplasms, especially adenomas, are one of the frequently occurring central nervous system (CNS) tumors, with a reported incidence of 6% to 10% of all intracranial tumors. Intraoperative consultation is often sought for, and crush preparations are utilized for the diagnostic purposes.
ANATOMY AND HISTOLOGY OF NORMAL PITUITARY GLAND
The adult human pituitary gland is housed in sella turcica, under the base of the brain. It is a bean-shaped organ, divided into two parts, anterior pituitary or adenohypophysis and posterior pituitary or neurohypophysis. The anterior pituitary is derived from Rathke’s pouch. The anterior pituitary constitutes the larger part of the gland, roughly 75% to 80%, and is formed by three components, namely the pars distalis, pars intermedia, and the pars tuberalis. The posterior pituitary is derived from the nervous system.
The pituitary gland measures approximately 13 × 9 × 6 mm and weighs about 0.6 g. It is surrounded by many important anatomic structures, relevant in differential diagnostic process.
Histologically, the anterior pituitary consists of acini, composed of eosinophilic, basophilic, and chromophobe cells in varying proportions. These represent specific cell types, each type associated with specific hormone production and function. The acini are surrounded by capillaryrich reticulin network.
Individual cell types can be correctly identified by immunohistochemical localization of the hormone products and ultrastructural morphology.
The neurohypophysis consists almost entirely of axonal terminations and accompanying glial cells (pituicytes) in a capillary-rich stroma.
PITUITARY ADENOMAS
Pituitary adenomas, derived from parenchymal cells of the adenohypophysis, are one of the most common benign neoplasms of the CNS.
CLASSIFICATION OF PITUITARY ADENOMAS
There are several classification systems for pituitary adenomas such as functional, anatomic or radiologic, histologic, immunohistochemical, and ultrastructural (Asa, 2011). The World Health Organization (WHO) classification of pituitary adenomas (2004) separates them into typical and atypical types and utilizes immunochemistry and ultrastructural examination, correlating them with clinical findings and specific hormone production.
The purpose of an intraoperative consultation is to identify the lesion as a pituitary neoplasm and not to subtype it. The specific histologic type requires ancillary studies. Therefore, this chapter is limited only to presenting the general cytopathologic features and the differential diagnosis.
CLINICAL FEATURES
Pituitary adenomas may be functional and symptomatic or nonfunctional. Approximately 25% of patients with pituitary adenomas lack a characteristic clinical syndrome or serum hormonal marker. Those without endocrine functions tend to present in a slightly older age group, usually after fifth decade, whereas adenomas with secretory activity arise between 30 and 50 years of age. They are uncommon in children under 12 years of age. Majority of the childhood pituitary adenomas are small and functional. The nonfunctional pituitary adenomas may be an incidental finding or cause symptoms due to the increased size.
The presenting symptoms caused by hormonal overproduction include amenorrhea, infertility, Cushing syndrome, and acromegaly. Those caused by compression of the surrounding tissues or organs include impaired eye movements, visual disturbances, nerve palsies, and compression of the optic chiasma.
An overwhelming majority of pituitary adenomas arise in the anterior hypophysis and are initially intrasellar. These tumors have a marked tendency to grow beyond the confines of pituitary fossa and occupy suprasellar or parasellar areas.
ASSOCIATION WITH HEREDITARY SYNDROMES
Up to 3% of the operated pituitary adenomas are associated with multiple neuroendocrine neoplasia syndrome, type 1 (MEN 1). See Chapter 1, Table 1.1.
RADIOGRAPHIC FINDINGS
Neuroimaging (CT or MRI) shows uniformly enhancing mass involving the pituitary gland.
GROSS AND MICROSCOPIC FEATURES
Grossly, most of the pituitary adenomas are solid and soft in consistency. Cystic change with hemorrhage is uncommon.
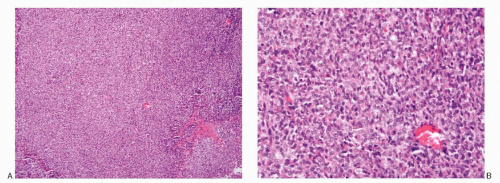
Microscopically, pituitary adenomas show a diffuse growth pattern consisting of sheets of uniform cells interrupted by delicate capillary network (Fig. 10.1). Perivascular location of neoplastic cells may result in the formation of pseudorosettes and pseudopapillary formation. The cells are small to medium sized and round. Their nuclei are typically uniform, round to oval, exhibiting a salt-pepper chromatin pattern. There is mild anisonucleosis, and distinct micronucleoli can usually be observed. The cell borders are well to poorly defined. The neoplastic cells demonstrate uniform tinctorial quality. Lack of stroma is characteristic. The cytoplasm can be eosinophilic or basophilic or amphophilic.
CYTOPATHOLOGIC FEATURES
The specimens represent tissue samples submitted for intraoperative consultation and processed by crush preparations. Due to lack of stroma, the tissue samples from pituitary adenomas easily produce a thin monolayered smear across the slide. The cytologic presentation is quite characteristic (Table 10.1; Figs. 10.2,10.3,10.4,10.5,10.6 and 10.7). The smears are usually quite cellular and composed of closely packed small- to medium-sized tumor cells, with high N/C ratios presenting a dispersed cell pattern. Pseudofollicular pattern is frequent. The adenoma cell nuclei are centrally placed, containing granular chromatin imparting a salt-pepper chromatin pattern, and small nucleoli. The cellular shapes may be round, oval, or polyhedral, and the cytoplasm in most instances is acidophilic or faintly basophilic. The tumors display abundant capillary sinusoids, and mitosis, necrosis, cellular pleomorphism, or cell processes are very seldom found.
Fig. 10.1: Histologic Sections of Pituitary Adenoma. A: Low-power view of a pituitary adenoma with a diffuse growth pattern (H&E). B: Higher magnification depicting a monotonous, small, round cell pattern. The cellular borders are poorly defined; the cytoplasm is eosinophilic and scant. The nuclei are round, containing finely granular chromatin, and micronucleoli are frequently present (H&E).
TABLE 10.1. CYTOPATHOLOGIC FEATURES OF PITUITARY ADENOMA
Scant, granular; eosinophilic, basophilic to amphophilic
Background
Granular due to spilled cytoplasmic contents; no necrosis
Immunoprofile
Neuroendocrine markers +; specific hormones
Ultrastructure
Pleomorphic secretory granules, variable in size, shape, numbers, and electron density
Differential diagnoses
Normal pituitary parenchyma
Metastatic poorly differentiated carcinoma
Plasmacytoma
Malignant lymphoma
Meningioma, small cell type
Paraganglioma
Hemangiopericytoma
Glioblastoma, small cell type
Oligodendroglioma
Central neurocytoma
Medulloblastoma
Peripheral neuroectodermal tumor (PNET)
Pineocytoma
Clear cell ependymoma
Nuclear monotony and minimal matrix are the rule. Tumors with trabecular architecture present short chains or circles of cells (Fig. 10.4A). The background may show diffuse granularity due to disruption of the cell borders and spillage of the cytoplasmic contents (Fig. 10.3D). Occasionally, the neoplastic cells may contain dense acidophilic cytoplasm (Fig. 10.4D), resembling oncocytes. The cytoplasmic granulation varies among the different subtypes, but uniform in a given tumor. Occasionally, the neoplastic cells are seen in small aggregates or balls (Figs. 10.3A and 10.4D). Scattered large nuclei may be seen (Fig. 10.6D,E).
IMMUNOPROFILE
The cells of pituitary adenomas are immunoreactive for synaptophysin and chromogranin and, apart from a few null cell adenomas, also express one or more of the pituitary hormones.
ULTRASTRUCTURE
Ultrastructurally, pituitary adenoma cells demonstrate secretory granules (sparsely granulated or densely granulated), which vary in terms of numbers, size, and shapes and electron density depending on the type of adenohypophysial cell. The secretory granules may be spherical, flattened, dented, heart shaped, teardrop shaped, or elongated. They vary from 150 to 700 nm in diameter, average being 150 to 400 nm. In some cells, the secretory granules demonstrate misplaced exocytosis (release of secretory material in intercellular space). Some demonstrate cytoplasmic processes (thyrotroph adenomas).
DIFFERENTIAL DIAGNOSES
Several neoplasms in the CNS are composed of small uniform cells and enter the differential diagnosis. The location of the lesions as well as clinical and radiologic data are critical.
The smears of the pituitary adenomas must be differentiated from normal pituitary parenchyma. The latter, because of its stromal content is extremely difficult to smear, resulting in thick tissue fragments that are difficult to visualize and interpret. This is in contrast to the samples from adenomas, which offer no resistance, allowing a smooth cell spread. If great pressure is used in smearing technique, the neoplastic cells may be crushed, deeply stained, and mistaken for metastatic small cell carcinoma. The differential diagnoses of pituitary adenoma include neoplasms with small round cells that occur in the sellar or parasellar area. They are listed in Table 10.2 and illustrated in Figs. 10.8,10.9,10.10,10.11,10.12,10.13,10.14,10.15,10.16,10.17 and 10.18. All the listed entities, although conceptually apply because of the round cell pattern, may not be applicable anatomically.
Only gold members can continue reading. Log In or Register to continue