Miscellaneous (Genitourinary, Head and Neck, Skin, Muscle, and Nervous System)
Miscellaneous (Genitourinary, Head and Neck, Skin, Muscle, and Nervous System)
2M01
Key word: Characteristics of Malignant Transformation of Nevi
Author: Joshua C. Grimm, MD
Editor: Lisa K. Jacobs, MD
A 39-year-old female has been followed regularly by her dermatologist for a mole located on her left shoulder. Due to a family history of melanoma and her fair complexion, she is concerned that this nevus might eventually progress to malignant disease. Which of the following is true concerning the malignant transformation from melanocytic nevus to frank melanoma?
Abnormal adhesion receptors make cells resistant to the typical progression from nevus to melanoma
All melanocytic nevi that change shape, color, or size are considered malignant
All melanomas arise from pre-existing nevi
Melanocytic nevi are not considered direct precursor lesions to melanoma
The BRAF mutation is found in a majority of patients with melanoma and nevi
Answer: (E) The BRAF mutation is found in a majority of patients with melanoma and nevi
Rationale:
The incidence of melanoma has risen in the past several decades. Screening consists of regular physical examinations, especially in those patients who have identifiable risk factors for and precursors to melanoma, such as melanocytic nevi. These lesions should be followed with regard to symmetry, border, color, size, and evolution over time, which may indicate that malignant transformation has occurred. However, it is important to note that histologic evidence, via a punch, incisional, or excisional biopsy, is necessary to diagnose an individual with melanoma.
A number of gene mutations have been identified as protooncogenes, which impact an individual’s risk of developing cancer. The BRAF gene is significant in melanoma. It codes for the BRAF protein, a protein kinase that modifies intracellular signaling as well as cell proliferation and differentiation. Alterations in these signaling pathways can allow tumor cells to evade the normal cell-cell adhesion controls that prevent melanocyte growth and invasion into surrounding tissues. Thus, a key component of malignant transformation is the expression of abnormal receptors that allow melanocytes to differentiate and expand unchecked.
References:
Li G, Herlyn M. Dynamics of intercellular communication during melanoma development. Mol Med Today. 2000;6(4): 163-169.
Pollock PM, Harper UL, Hansen KS, et al. High frequency of BRAF mutations in nevi. Nat Genet. 2003;33(1):19-20.
Tsao H, Bevona C, Goggins W, et al. The transformation rate of moles (melanocytic nevi) into cutaneous melanoma: A population-based estimate. Arch Dermatol. 2003;139(3): 282-288.
Zaal LH, Mooi WJ, Klip H, et al. Risk of malignant transformation of congenital melanocytic nevi: A retrospective nationwide study from The Netherlands. Plast Reconstr Surg. 2005; 116(7):1902-1909.
2M02
Key word: Complication of Late Reduction of Posterior Hip Dislocation
Author: Raja Mohan, MD
Editor: Frank J. Frassica, MD
A 20-year-old man was an unrestrained passenger in a motor vehicle collision. Upon impact, his left leg hit the dashboard and caused a posterior hip dislocation. This was reduced in the emergency department approximately 20 hours after the accident. What is the most likely complication?
A number of complications can occur with hip dislocations, but the two most common are hip arthritis and avascular necrosis of the femoral head. The risk of these complications increases when reduction of the dislocation is performed late. After reduction, an MRI should be performed to rule out avascular necrosis of the femoral head. The incidence is approximately 15% in patients who had a posterior hip dislocation.
Reference:
McKee MD, Garay ME, Schemitsch EH, et al. Irreducible fracture-dislocation of the hip: A severe injury with a poor prognosis. J. Orthop Trauma. 1998;12(4):223-229.
2M03
Key word: Concomitant Injury with Bilateral Calcaneal Fractures
Author: Isaac Howley, MD
Editor: Frank J. Frassica, MD
A 30-year-old male is brought to the emergency room after falling off a second story balcony and landing on both feet before striking his head. He arrives intubated with normal hemodynamic parameters and a Glasgow Coma Scale score of 6T (withdraws to pain). His physical examination reveals bilateral swollen, erythematous heels but is otherwise free of other obvious deformities. In addition to computed tomography (CT) imaging of his head, cervical spine, abdomen, and pelvis, and x-rays of his chest and bilateral feet, what other plain film imaging should be obtained?
Calcaneal fractures are relatively rare fractures that typically occur in young patients following motor vehicle collisions or falls from significant height onto the feet. The force of impact is frequently transmitted not only from the ground onto the patient’s hindfoot, but also along the vertical axis in an axial load injury pattern. Calcaneal fractures are bilateral or are accompanied by lumbar spine fractures 10% to 15% of the time; anteroposterior and lateral plain films of the lumbar spine should therefore be obtained routinely. Other common accompanying injuries include fractures of the tibial plateau, proximal femur, and pelvis. These bones should be carefully assessed as part of the secondary or tertiary survey in patients who present with calcaneal fractures, and a low threshold should be maintained for obtaining radiographic studies.
Calcaneal fractures involve the subtalar joint approximately 75% of the time. Thin slice (2 to 3 mm) CT imaging is useful in defining the fracture anatomy. When uncorrected, calcaneal fractures may cause permanent and debilitating widening of the heel, making it difficult for patients to wear shoes. Edema can be significant, and compartment syndrome of the foot may occur in 10% of cases, warranting careful monitoring for this complication. Controversy remains as to the relative merits of operative and nonoperative management. Although nonoperative management can cause significant disability, operative management is frequently plagued by complications, especially with wound healing. Patient factors such as smoking, age, and medical comorbidities play a large role in the risk for operative complications and should be taken into account in treatment decision making.
Patterns of Injury to the Head, Neck, Trunk, and Extremities Associated with Orthopedic Injuries
Key word: Diagnostic Findings of Digital Paresthesias
Author: Raja Mohan, MD
Editor: Frank J. Frassica, MD
A 34-year-old woman presents with pain in her right hand and neck that has been going on for 1 year. She experiences occasional numbness in her arm and hand. She works as a seamstress and reports that her symptoms are worsened when shooting a basketball. What is the most likely diagnosis?
Thoracic outlet syndrome is a condition that can cause impingement or irritation of the subclavian artery, subclavian vein, or brachial plexus. Neurologic findings are the most common symptoms seen in those with symptomatic thoracic outlet syndrome. Neurologic findings can include numbness, tingling, or weakness in the patient’s neck, shoulders, or arm. Thoracic outlet syndrome can be caused by a cervical rib, trauma, enlarged scalene muscle, or narrowing between the clavicle and the first rib.
Carpal tunnel syndrome is only confined to the hand, and medial epicondylitis only involves the medial forearm. Any neck or upper arm symptoms rule out these conditions. Brachial plexopathy can cause pain or paresthesia but would not explain why the patient in this vignette has worse symptoms while playing basketball. Patients with thoracic outlet syndrome tend to have exacerbation of symptoms when raising their arms above their head.
Key word: Diagnosis of Paralysis of the Common Peroneal Nerve
Author: Raja Mohan, MD
Editor: Frank J. Frassica, MD
A 25-year-old man was involved in a motor vehicle accident and suffered a tibial plateau fracture that was splinted in the emergency department. Several days after admission he develops difficulty with dorsiflexion of his foot and also reports numbness and tingling sensations in the injured leg. In which region of the leg would he most likely feel numbness and tingling?
The common peroneal (fibular) nerve gives rise to two branches: The superficial peroneal nerve and the deep peroneal nerve. This nerve can be compressed by a lower extremity splint and begin to cause sensory and motor deficits. The superficial peroneal nerve provides cutaneous sensation to the dorsum of the foot and all digits except the lateral portion of the fifth digit and the first web space. The deep peroneal nerve provides cutaneous sensation to the first web space. On the plantar surface or sole of the foot, the medial and lateral plantar nerves (terminal branches of the tibial nerve) provide cutaneous sensation to the medial and lateral portions of the plantar surface, respectively. The cutoff between these two regions is a line drawn from the middle of the fourth digit of the foot. The saphenous nerve (branch of the femoral nerve) provides cutaneous sensation for the medial malleolus, and the sural nerve for the lateral malleolus.
Injury to the common peroneal nerve also results in difficulty with dorsiflexion—foot drop. The superficial peroneal nerve innervates the muscles of the lateral compartment (peroneus longus, peroneus brevis) of the leg, whereas the deep peroneal nerve innervates the muscles of the anterior compartment (tibialis anterior, extensor hallucis longus, extensor digitorum longus, peroneus tertius) of the leg. The anterior compartment of the leg is responsible for dorsiflexion of the foot, and therefore foot drop can result from peroneal nerve compression.
A 25-year-old male notices a painless mass in his scrotum for the first time while showering. Which of the following is an accurate statement regarding the diagnosis of testicular masses?
Biopsy of the testicle is generally required prior to radical inguinal orchiectomy in order to provide a histologic diagnosis
Cystic or fluid-filled masses detected on scrotal ultrasound are typically seminomas
Physical examinations can be performed less frequently with the availability of scrotal ultrasounds
Scrotal ultrasound can distinguish extrinsic from intrinsic testicular lesions and can detect intratesticular lesions as small as 1 to 2 mm
Transillumination studies are sufficient in discerning between malignant versus benign testicular masses
Answer: (D) Scrotal ultrasound can distinguish extrinsic from intrinsic testicular lesions and can detect intratesticular lesions as small as 1 to 2 mm.
Rationale:
Testicular cancer is the most common solid malignancy in men of 15 to 35 years of age. All solid testicular masses discovered on physical examination and documented on ultrasound are malignant until proven otherwise. Initial studies must include physical examination, ultrasound, and tumor markers, such as alpha fetoprotein and β-human chorionic gonadotropin. Ultrasound can distinguish extrinsic from intrinsic lesions with great accuracy and can detect lesions as small as 1 mm. A fluid-filled or cystic mass is unlikely to represent malignancy. Nonseminomatous germ cell tumors typically appear heterogenous with calcifications, cystic areas, and indistinct margins. Seminomas appear as well-defined hypoechoic lesions without cystic areas. Scrotal ultrasound has become an extension of the physical examination but should not be a substitute for the latter.
Chest and abdominal imaging with computed tomography (CT) or magnetic resonance imaging (MRI) should be performed to evaluate for metastasis. There is no role for percutaneous biopsy of testicular masses due to the risk of altering the natural retroperitoneal lymphatic drainage of the testicles and seeding the scrotal wall. Radical inguinal orchiectomy is used to provide both histologic diagnosis and local tumor control.
References:
Benson CB. The role of ultrasound in diagnosis and staging of testicular cancer. Semin Urol. 1988;6(3):189-202.
Rochelle LJ, Schuch B, Belldegrun A. Urology. In: Brunicardi FC, ed. Schwartz’s Principles of Surgery. 9th ed. New York, NY: McGraw-Hill; 2010:1462.
2M07
Key word: Ethical Issues in Injury Prevention
Authors: Lisa M. Kodadek, MD, and Kyle J. Van Arendonk, MD, PhD
Editor: Kent A. Stevens, MD, MPH
A 17-year-old woman brings her 11-month-old infant boy to the emergency department for seizure activity. Despite no report of trauma, the child has a bruise on his scalp and is found to have a subarachnoid hemorrhage on computed tomography. Which of the following is true with regard to the potential for nonaccidental injury?
Head injury is the most common manifestation of nonaccidental injury
Nonaccidental injury is seen similarly across parent age and socioeconomic status
Nonaccidental injury is the most common cause of hemorrhagic stroke in children
Skeletal survey is unnecessary in this patient
This patient should undergo ophthalmologic examination
Answer: (E) This patient should undergo ophthalmologic examination
Rationale:
Physical abuse, or nonaccidental injury, is unfortunately quite common in children. Nonaccidental injury can occur in any child but is more common among boys, children under 2 years of age, children born to young mothers, children living in poverty, and children with special needs.
Providers must be aware of clues suggesting nonaccidental injury, such as a lack of explanation for an injury, an injury severity that is incompatible with the reported mechanism, a changing report of what happened, and delay in seeking medical care. Any incident of suspected nonaccidental injury must be reported to allow for a thorough investigation with the assistance of child protection services.
The most common manifestation of nonaccidental injury is bruising and other soft tissue injuries. Multiple bruises of various colors and in unusual locations and soft tissue injuries matching specific instruments (belt, etc.) may be seen. The second most common manifestation of nonaccidental injury is fracture. In children with other evidence of abuse or with a suspicious fracture, such as a femoral fracture in a non-ambulatory child, a skeletal survey should be performed to search for other fractures. Multiple fractures at various stages of healing are especially concerning for nonaccidental injury.
Abusive head trauma may present with intracranial hemorrhage with no apparent history of trauma. Other findings consistent with abusive head trauma include scalp or ear bruising, retinal hemorrhages in multiple retinal layers, and chronic failure to thrive. Retinal hemorrhages are common in nonaccidental trauma but not in accidental trauma, and therefore ophthalmologic examination is an important component in any abuse investigation. Although a high level of suspicion is important given the morbidity and mortality associated with abusive head trauma, it is also important not to presume that a child’s presentation is secondary to abuse unless there is specific evidence to warrant concern. The most common cause of hemorrhagic stroke in children is in fact arteriovenous malformation rather than nonaccidental injury.
Reference:
Keenan HT, Runyan DK, Marshall SW, et al. A population-based study of inflicted traumatic brain injury in young children. JAMA. 2003;290(5):621-626.
2M08
Key word: Etiology of Secondary Traumatic Brain Injury
Author: Isaac Howley, MD
Editor: Albert Chi, MD
An 11-year-old boy presents to the emergency department after falling out of a tree at a height of approximately 6.1 m (20 ft). His primary survey is negative. On secondary survey, you note a Glasgow Coma Scale (GCS) score of 12, tenderness and rigidity of his abdomen, and extremity injuries. Computed tomography scans of his head, abdomen, and pelvis reveal an occipital subarachnoid hemorrhage and a grade 2 splenic laceration. Which of the following is true with regard to secondary brain injury?
According to the Monro-Kellie doctrine, the cranial vault is a closed space, and thus an increase in one constituent volume must be compensated by reduction in another constituent volume
All patients with moderate or severe brain injuries should have an intracranial pressure monitor placed
Answer: (A) According to the Monro-Kellie doctrine, the cranial vault is a closed space, and thus an increase in one constituent volume must be compensated by reduction in another constituent volume
Rationale:
Traumatic brain injury may be divided into two phases: Primary and secondary. Primary injury is a result of the transfer of mechanical force in the initial traumatic episode and includes skull fractures, hematoma formation, and diffuse axonal injuries. Primary injuries may consist of both coup and opposite contrecoup injuries, in which the brain’s momentum causes it to strike the side of the calvarium opposite the original impact. The Monro-Kellie doctrine states that the cranial vault is a closed space; the volume increase due to hemorrhage or cerebral edema must be compensated by decrease in other volumes such as intravascular blood. Secondary injury occurs when this compensation becomes pathologic.
Multiple maneuvers may be attempted to improve cerebral perfusion pressure (CPP) by maintaining mean arterial pressure (MAP) and mitigating increases in intracerebral pressure (ICP). Patients with severe brain injuries (GCS score <9) should be considered for placement of an ICP monitor to guide therapy. The head of the bed should be elevated to 30 degrees, and hypertonic saline and mannitol may be given to reduce cerebral edema and thus ICP. Hyperventilation causes intracerebral vasoconstriction, reducing intracerebral blood volume, and thus ICP; however, it also reduces cerebral blood flow, potentially worsening hypoxia. Steroids have not been shown to be effective in prevention of secondary injury.
Reference:
Patterson JT, Hanbali F, Franklin RL, et al. Neurosurgery. In: Townsend CM, Beauchamp RD, Evers BM, Mattox KL, eds. Sabiston Textbook of Surgery. 18th ed. Philadelphia, PA: Saunders Elsevier; 2008:2112-2115.
2M09
Key word: Etiology of Bleeding Pelvic Fractures
Author: Jens U. Berli, MD
Editor: Albert Chi, MD
A 42-year-old male construction worker is brought to the emergency room after a 120-kg concrete plate landed on his lower anterior torso. The patient has a heart rate of 110 beats per minute and blood pressure of 95/55 mm Hg. His pelvis is unstable on examination, and you temporarily stabilize the pelvis using a binder and complete your assessment, which is otherwise negative. His vital signs respond only transiently to crystalloid resuscitation. You decide to take him to the angiography suite for potential pelvic embolization. What is the most likely source of hemorrhage in this patient?
Pelvic fractures are a difficult to manage entity in trauma and orthopedic surgery. The patient described above suffered from an anterior to posterior compression-type fracture. It is mentioned that the fracture is unstable so likely one or both of his sacroiliac joints are disrupted. The most prevalent arteries to be injured during such a mechanism are the superior gluteal (due to its relation to the sharp fascia of the piriformis and the sacroiliac joint, see figure) and the internal pudendal (runs through pelvic floor with its ligaments, see figure).
Internal iliac plexus of arteries and veins. Reprinted with permission from: Tile R. Anatomy of the pelvic ring. In: Tile M, Helfet DL, Kellam JF, eds. Fractures of the Pelvis and Acetabulum. 3rd ed. Philadelphia, PA: Lippincott Williams & Wilkins, 2003.
Arterial injuries are present in about 5% to 10% of pelvic fractures. By far the most common source of bleeding is venous from bridging veins and osseous surfaces. This form responds relatively well to pelvic binding with reapproximation of the anatomy. If the peritoneum is intact, the retroperitoneum helps to tamponade venous bleeding. In this patient, signs of continued bleeding despite correct pelvic binding and without any signs of intraperitoneal blood loss make arterial bleeding the highest concern on the differential until proven otherwise.
Knowledge of anatomy, fracture classification, presentation, and initial management are crucial to good outcome in this population. Early mortality from pelvic fractures in firstworld countries is still around 5% to 10%. Initial management is directed at hemostasis, pelvic stabilization, and urogenital assessment. For active bleeding, treatment options are pelvic binding, angiography, and preperitoneal pelvic packing, typically escalating in the order provided. Angiography requires a fluid-responsive patient. If the patient cannot be stabilized, emergent preperitoneal pelvic packing with external pelvic stabilization is the safest option.
References:
Ben-Menachem Y, Coldwell DM, Young JW, et al. Hemorrhage associated with pelvic fractures: Causes, diagnosis, and emergent management. AJR Am J Roentgenol. 1991; 157(5):1005-1014.
Burlew CC, Moore EE, Smith WR, et al. Preperitoneal pelvic packing/external fixation with secondary angioembolization: Optimal care for life-threatening hemorrhage from unstable pelvic fractures. J Am Coll Surg. 2011;212(4):628-635; discussion 635-637.
Hak DJ, Smith WR, Suzuki T. Management of hemorrhage in life-threatening pelvic fracture. J Am Acad Orthop Surg. 2009;17(7):447-457.
2M10
Key word: Findings with Temporal Bone Fractures
Author: Lisa M. Kodadek, MD
Editor: Albert Chi, MD
A 23-year-old man presents after sustaining blunt head trauma during a physical altercation. He is noted to have drooping of his right nasolabial fold and inability to wrinkle his right forehead or close his right eye. The most likely cause of his symptoms is:
The most common causes of facial nerve injury are temporal bone fractures, penetrating injuries, and iatrogenic injuries. Injury of the facial nerve in temporal bone fractures can result from bony fragment compression, intraneural hematoma, or loss of nerve continuity. Parietal bone fractures are not associated with facial nerve injury. The patient’s symptoms are consistent with Bell palsy but given his clinical history, temporal bone fracture is a more likely etiology. Intracranial malignancy is a less likely cause of facial nerve paralysis. Stroke may have a similar presentation but would be unlikely in a young person without any risk factors. Furthermore, motor innervation to the forehead is typically preserved in stroke.
Reference:
Mattox DE. Clinical disorders of the facial nerve. In: Flint PW, Haughey BH, Lund VJ, Niparko JK, Richardson MA, Robbins KT, Thomas JR, eds. Cummings Otolaryngology: Head & Neck Surgery. 5th ed. Philadelphia, PA: Mosby Elsevier; 2010:2391-2402.
2M11
Key word: Fracture Associated with Major Vascular Compromise
Author: Raja Mohan, MD
Editor: Ying Wei Lum, MD
A 12-year-old boy tripped and fell on his outstretched right hand. Upon presentation to the emergency department, the boy has a swollen and extremely tender right elbow. On physical examination, the hand appears warm, but the radial pulse is absent. An x-ray reveals a displaced supracondylar humerus fracture. What is the next step in management of this patient?
Closed reduction of fracture with application of a splint
Answer: (A) Closed reduction of fracture with application of a splint
Rationale:
Supracondylar fractures in children are very common and usually occur following a fall with an outstretched arm. Neurovascular injury can occur as a result of stretch injury with such fractures. Fortunately, the pulse frequently returns after reduction of the fracture, and thus reduction of the fracture and application of a splint is recommended when patients have a warm, well-perfused hand despite the absence of a palpable pulse. Direct vascular injury is uncommon, but if it does happen, immediate operative repair is required.
Reference:
White L, Mehlman CT, Crawford AH. Perfused, pulseless, and puzzling: A systematic review of vascular injuries in pediatric supracondylar humerus fractures and results of a POSNA questionnaire. J Pediatr Orthop. 2010;30(4): 328-335.
2M12
Key word: Human Factors in Injury Prevention
Author: Lisa M. Kodadek, MD
Editor: Kent A. Stevens, MD, MPH
A trimodal distribution exists for mortality after traumatic injury. How can mortality during the first mortality peak best be prevented?
Early intubation and mechanical ventilation
Early operative intervention
Injury prevention and control strategies
Prehospital resuscitation with intravenous fluids
Transport to a level one trauma center within 1 hour of injury
Answer: (C) Injury prevention and control strategies
Rationale:
A trimodal distribution for mortality exists after traumatic injury. The first mortality peak is within seconds or minutes of injury and accounts for half of all trauma deaths. These deaths result from injury to the aorta, heart, brainstem, spinal cord, or acute respiratory distress. The only proven way to prevent death among patients in this first mortality peak is through injury prevention and control practices such as seatbelt use; helmet use; airbags; antilock brakes; laws to prevent intoxicated and impaired drivers; speed limit laws; and improved road lighting, signage, and safety design.
The second mortality peak occurs within hours of injury and accounts for approximately 30% of trauma deaths. These patients are best served by rapid transport to a level one trauma center within the so-called “golden hour.” Prehospital resuscitation and early operative intervention may also be of benefit to this subset of trauma patients. The third mortality peak occurs greater than 24 hours after injury and typically is caused by infection or multiple organ failure. Early intubation and mechanical ventilation have an important role in treating these patients with sepsis or respiratory failure after injury.
Only gold members can continue reading. Log In or Register to continue
 Abnormal adhesion receptors make cells resistant to the typical progression from nevus to melanoma
Abnormal adhesion receptors make cells resistant to the typical progression from nevus to melanoma All melanocytic nevi that change shape, color, or size are considered malignant
All melanocytic nevi that change shape, color, or size are considered malignant All melanomas arise from pre-existing nevi
All melanomas arise from pre-existing nevi Melanocytic nevi are not considered direct precursor lesions to melanoma
Melanocytic nevi are not considered direct precursor lesions to melanoma The BRAF mutation is found in a majority of patients with melanoma and nevi
The BRAF mutation is found in a majority of patients with melanoma and nevi Avascular necrosis of femoral head
Avascular necrosis of femoral head Femoral head fracture
Femoral head fracture Heterotopic ossification
Heterotopic ossification Sciatic nerve injury
Sciatic nerve injury Shortening of leg
Shortening of leg Bilateral ankles, thoracic spine, lumbar spine
Bilateral ankles, thoracic spine, lumbar spine Bilateral ankles, tibia/fibula, femurs, lumbar spine, thoracic spine
Bilateral ankles, tibia/fibula, femurs, lumbar spine, thoracic spine Bilateral ankles, tibia/fibula, femurs, pelvis, lumbar spine
Bilateral ankles, tibia/fibula, femurs, pelvis, lumbar spine Bilateral ankles, tibia/fibula, femurs, pelvis, thoracic spine
Bilateral ankles, tibia/fibula, femurs, pelvis, thoracic spine Bilateral ankles, tibia/fibula, lumbar spine
Bilateral ankles, tibia/fibula, lumbar spine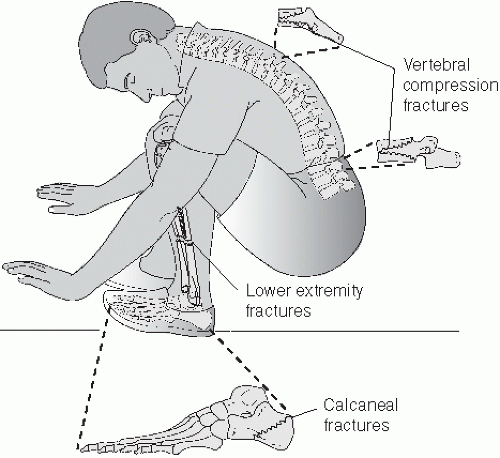
 Brachial plexopathy
Brachial plexopathy Carpal tunnel syndrome
Carpal tunnel syndrome Complex regional pain syndrome
Complex regional pain syndrome Medial epicondylitis
Medial epicondylitis Thoracic outlet syndrome
Thoracic outlet syndrome Dorsum of foot
Dorsum of foot Lateral plantar surface of foot
Lateral plantar surface of foot Medial plantar surface of foot
Medial plantar surface of foot Over lateral malleolus
Over lateral malleolus Over medial malleolus
Over medial malleolus Biopsy of the testicle is generally required prior to radical inguinal orchiectomy in order to provide a histologic diagnosis
Biopsy of the testicle is generally required prior to radical inguinal orchiectomy in order to provide a histologic diagnosis Cystic or fluid-filled masses detected on scrotal ultrasound are typically seminomas
Cystic or fluid-filled masses detected on scrotal ultrasound are typically seminomas Physical examinations can be performed less frequently with the availability of scrotal ultrasounds
Physical examinations can be performed less frequently with the availability of scrotal ultrasounds Scrotal ultrasound can distinguish extrinsic from intrinsic testicular lesions and can detect intratesticular lesions as small as 1 to 2 mm
Scrotal ultrasound can distinguish extrinsic from intrinsic testicular lesions and can detect intratesticular lesions as small as 1 to 2 mm Transillumination studies are sufficient in discerning between malignant versus benign testicular masses
Transillumination studies are sufficient in discerning between malignant versus benign testicular masses Head injury is the most common manifestation of nonaccidental injury
Head injury is the most common manifestation of nonaccidental injury Nonaccidental injury is seen similarly across parent age and socioeconomic status
Nonaccidental injury is seen similarly across parent age and socioeconomic status Nonaccidental injury is the most common cause of hemorrhagic stroke in children
Nonaccidental injury is the most common cause of hemorrhagic stroke in children Skeletal survey is unnecessary in this patient
Skeletal survey is unnecessary in this patient This patient should undergo ophthalmologic examination
This patient should undergo ophthalmologic examination According to the Monro-Kellie doctrine, the cranial vault is a closed space, and thus an increase in one constituent volume must be compensated by reduction in another constituent volume
According to the Monro-Kellie doctrine, the cranial vault is a closed space, and thus an increase in one constituent volume must be compensated by reduction in another constituent volume All patients with moderate or severe brain injuries should have an intracranial pressure monitor placed
All patients with moderate or severe brain injuries should have an intracranial pressure monitor placed Hyperventilation decreases PCO2, causing intracranial vasodilation and thus increased cerebral blood flow
Hyperventilation decreases PCO2, causing intracranial vasodilation and thus increased cerebral blood flow Steroids have been proven to reduce the risks of herniation and death in patients with severe brain injuries
Steroids have been proven to reduce the risks of herniation and death in patients with severe brain injuries The brain matter 180 degrees away from the site of primary brain injury is at risk for a secondary contrecoup injury
The brain matter 180 degrees away from the site of primary brain injury is at risk for a secondary contrecoup injury Bridging veins in the pelvis
Bridging veins in the pelvis Common iliac artery
Common iliac artery Internal iliac artery
Internal iliac artery Internal iliac vein
Internal iliac vein Superior gluteal artery
Superior gluteal artery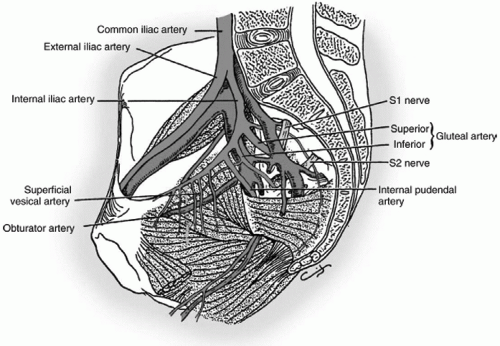
 Bell palsy
Bell palsy Intracranial malignancy
Intracranial malignancy Parietal bone fracture
Parietal bone fracture Stroke
Stroke Temporal bone fracture
Temporal bone fracture Closed reduction of fracture with application of a splint
Closed reduction of fracture with application of a splint External fixation of fracture
External fixation of fracture Observation
Observation Operative exploration for vascular injury
Operative exploration for vascular injury Place in splint
Place in splint Early intubation and mechanical ventilation
Early intubation and mechanical ventilation Early operative intervention
Early operative intervention Injury prevention and control strategies
Injury prevention and control strategies Prehospital resuscitation with intravenous fluids
Prehospital resuscitation with intravenous fluids Transport to a level one trauma center within 1 hour of injury
Transport to a level one trauma center within 1 hour of injury


