Minimally Invasive Video-Assisted Thyroidectomy
Paolo Miccoli
Gabriele Materazzi
DEFINITION
Minimally invasive video-assisted thyroidectomy (MIVAT) is an endoscopic procedure characterized by the use of external retraction, avoiding any gas inflation, in order to create an operative space in the neck.
This approach to the thyroid has been used at our Department of Surgery for the last 15 years on more than 3,500 patients with results that can successfully rival those of standard open surgery.
This is not an appropriate operation for any patient with thyroid disease; patients must be strictly selected. Only 10% to 30% of the cases1 are appropriate for a MIVAT procedure.
PATIENT HISTORY AND PHYSICAL FINDINGS
The inclusion criteria and the main contraindications are summarized in the following text. The most significant limit is represented by the size of both the nodule(s) and/or the gland as measured by means of an accurate ultrasonographic study obtained preoperatively. In countries where goiter is endemic, the gland volume can be relevantly independent from the nodule volume, and this aspect might be responsible for the necessity of converting the procedure.
Ultrasonography can also be useful to exclude the presence of thyroiditis, which might make the dissection troublesome. In case ultrasonography only gives the suspicion of thyroiditis, autoantibodies should be measured in the serum. If thyroiditis is diagnosed preoperatively, this is a consideration to MIVAT.
One of the most controversial aspects regarding the appropriateness of MIVAT is in the treatment of malignant thyroid disease. “Low-risk” papillary carcinoma constitutes an ideal indication for MIVAT,2,3 but it is important to take into account the possibility of lymph node involvement in the neck. Great caution should be taken when there is the possibility of either metastatic lymph nodes or extracapsular invasion of the gland, both of which represent a contraindication to the minimally invasive endoscopic procedure.
Indications
Multinodular goiter (thyroid volume less than 25 mL and nodules smaller than 3 cm)
Low-risk papillary carcinoma
Graves’ disease
Microfollicular/Hürthle cell adenoma
RET gene mutation carriers (familial medullary thyroid carcinoma)
Contraindications
Absolute
Previous neck surgery
Acute thyroiditis
Metastatic carcinoma (levels II to VI)
Locally advanced carcinoma
Sporadic medullary carcinoma
Relative
Previous neck irradiation
Short neck in an obese patient
Chronic thyroiditis
IMAGING AND OTHER DIAGNOSTIC STUDIES
All patients should undergo (1) neck ultrasound in order to evaluate thyroid gland total volume (this should be less than 25 mL) and diameter of nodule/s (these should be less than 3 cm); (2) fine needle aspiration cytology of suspicious nodules; (3) blood tests in order to exclude thyrotoxicosis and acute thyroiditis before surgery; (4) basal serum calcitonin dosage is strongly suggested in order to exclude medullary carcinoma, which is a contraindication to MIVAT; (5) routine preoperative laryngoscopy is strongly recommended in all patients in order to identify asymptomatic vocal cord palsy.
TECHNIQUES
POSITIONING OF THE PATIENT AND DRAPING
Patient is positioned in supine position without neck extension (FIG 1). Hyperextension must be avoided because it would reduce the operative space. Conventional neck preparation and draping is obtained. The skin is protected by means of a sterile film (Tegaderm®).
 FIG 1 • Position of the patient on the operative table: Neck is not extended and skin is covered by sterile drapes. |
POSITIONING OF THE SURGICAL TEAM
Operation is performed by four surgeons: The first surgeon is on the right side of the table, the first assistant is on the left side of the table. The second assistant, who is holding the retractors, is at the head of the table. The third assistant, who is holding the endoscope, is on the left side of the table.The scrub nurse is behind the surgeon on the right side of the table (FIG 2).
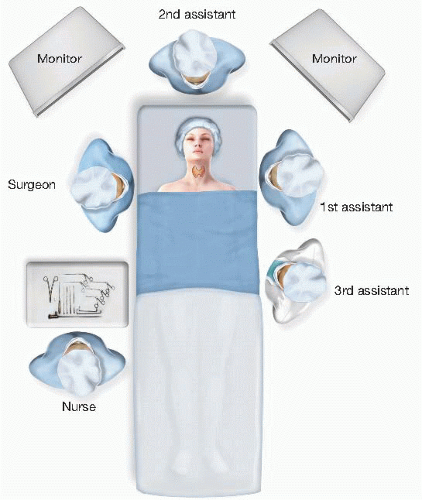 FIG 2 • Operating room setup: Team ▪ The surgeon is on the right side of the table. ▪ The first assistant is on the left side of the table (opposite the surgeon). ▪ The second assistant is at the head of the table. ▪ The third assistant is on the left side of the table. ▪ The scrub nurse is behind the surgeon on the right side of the table. |
INSTRUMENTATION
Forward-oblique telescope 30 degrees, diameter 5 mm, length 30 cm; suction dissector with cutoff hole, with stylet, blunt, length 21 cm; ear forceps, very thin, serrated, working length 12.5 cm; conventional tissue retractor army navy type; small tissue retractor, double-ended, length 12 cm; clip applier for vascular clips; straight scissors, length 12.5 cm, Harmonic Scalpel CS14; electrocautery (monopolar) (FIG 3).
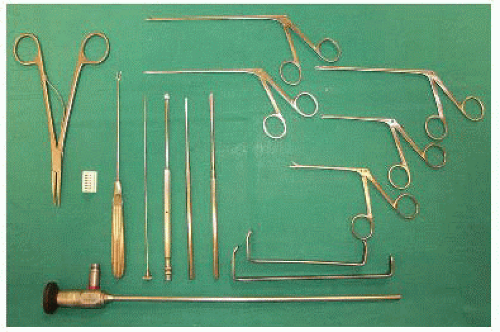 FIG 3 • Instrumentation for MIVAT. |
INCISION AND PREPARATION OF THE OPERATIVE SPACE
A 1.5-cm horizontal skin incision is performed 2 cm above the sternal notch in the central cervical area (FIG 4). Subcutaneous fat and platysma are carefully dissected so as to avoid any minimum bleeding.
Two small retractors are used to expose the midline, which has to be incised for 2 to 3 cm in an absolutely bloodless plane (FIG 5).
The blunt dissection of the thyroid lobe from the strap muscles is performed through the skin incision by gentle retraction and using tiny spatulas. When the thyroid lobe is almost completely dissected from the strap muscles,
larger and deeper retractors (army navy type) can be inserted and they will maintain the operative space during all the endoscopic part of the procedure (FIG 6).
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


