Metastatic Tumors
Dina R. Mody, MD
Key Facts
Clinical Issues
Most common primary sites are lung, breast, prostate, kidney, and thyroid
Predilection for regions containing red marrow
Commonly involved bones include skull, spine, ribs, pelvis, humerus, and femur
Pain is typical presenting symptom of skeletal metastases
Cytopathology
Usually cellular; however, can be bloody and hypocellular
Epithelial, cohesive cells in carcinomas
Crush effect and chromatin streaking: Think small cell carcinoma/lymphoma
Clear cells: Consider renal cell, lung
In general, metastases try to imitate primary
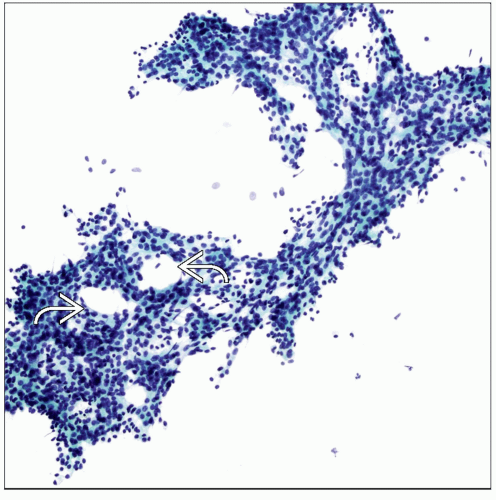 Pap stain of metastatic prostate carcinoma shows cribriform pattern characterized by punched-out intrasheet lumina  . The cells are cohesive in sheets and clearly do not belong in the bone. . The cells are cohesive in sheets and clearly do not belong in the bone. |
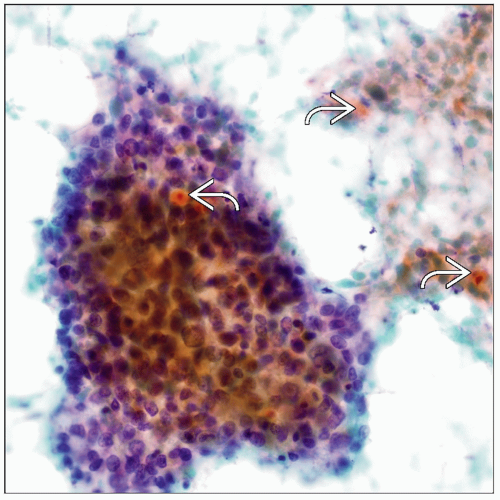 Pap stain shows a large syncytial cluster of malignant cells with abrupt keratinization  that indicates the squamous nature of this poorly differentiated carcinoma. that indicates the squamous nature of this poorly differentiated carcinoma. |
CLINICAL ISSUES
Epidemiology
Incidence
Far more common than primary bone tumors (25:1)
Most common primary sites are lung, breast, prostate, kidney, and thyroid
Other tumors include lymphoma, melanoma, neuroendocrine carcinoma (NEC), and hepatocellular carcinoma
Rarely, osteosarcoma shows bone-to-bone metastasis
After lungs and liver, skeleton is 3rd most frequent site of metastatic disease
˜ 40-90% of patients with advanced carcinoma have skeletal metastases during course of disease
Age
More common in elderly population
Site
Predilection for regions containing red marrow
Commonly involved bones include skull, spine, ribs, pelvis, humerus, and femur
Metastases distal to knee and tibia are rare
Distal metastases are typically from lung
In long bones, metastatic deposits tend to involve metaphysis
Solitary metastasis in long bones may mimic primary sarcoma
Presentation
Pain is a typical presenting symptom of skeletal metastases
Pathologic fracture
Neurological symptoms with spinal metastasis
Treatment
Surgical approaches
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


