Metastatic Malignant Melanoma
Key Facts
Clinical Issues
Lung is frequent site of metastasis for malignant melanoma
Middle-aged to elderly patients
Image Findings
Multiple, well-defined nodules in periphery of lungs
Endobronchial metastases
Microscopic Pathology
Can show large variety of morphologic appearances, including epithelioid, spindle, signet ring cell, rhabdoid, and small cell melanoma
Hallmark of malignant melanoma is presence of cells with marked cytologic atypia
Majority of tumor cells are large, pleomorphic, with enlarged nuclei and prominent eosinophilic nucleoli
Cells may also be small and relatively bland-appearing with minimal cytologic atypia
Ancillary Tests
S100 protein is positive in nearly 100% of cases (nuclear and cytoplasmic stain)
In most cases, melanocytic-associated markers are positive: HMB-45, Melan-A, tyrosinase, microphthalmia transcription factor (MiTF)
Aberrant expression of epithelial markers (keratins, CEA, EMA) can be seen in small percentage of cases
Other markers can also be expressed, including CD10, CD56, CD68, CD99, CD117, calretinin, NSE, vimentin, and Bcl-2, but are nonspecific
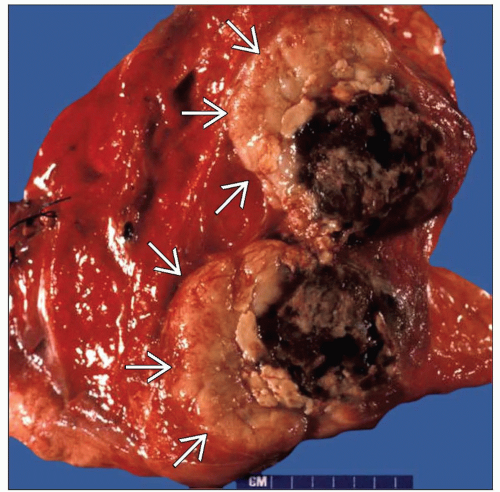 Gross appearance of a bisected nodule  containing a lung metastasis of malignant melanoma shows a well-circumscribed tan nodule with an area of black discoloration due to melanin pigment deposition. containing a lung metastasis of malignant melanoma shows a well-circumscribed tan nodule with an area of black discoloration due to melanin pigment deposition. |
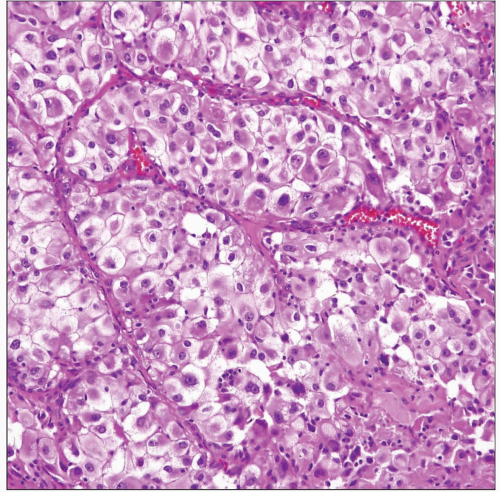 Histologic appearance of metastatic malignant melanoma in the lung shows nests of large, epithelioid tumor cells with enlarged nuclei, prominent nucleoli, and abundant eosinophilic cytoplasm. |
CLINICAL ISSUES
Epidemiology
Incidence
Lung is frequent site of metastasis for malignant melanoma
Age
Middle-aged to elderly patients
Presentation
Cough
Hemoptysis
Dyspnea
Atelectasis
Pleural effusion
Treatment
Surgical approaches
Surgical excision for solitary lesions may improve median survival
Adjuvant therapy
Chemotherapy may be used for multiple and bilateral tumors
Prognosis
Melanoma metastases to lungs are associated with advanced stage and poor prognosis
IMAGE FINDINGS
General Features
Location
Multiple, well-defined nodules in periphery of lungs
Endobronchial metastases
Morphology
Round, well-defined nodules
Can show cavitation and necrosis
MACROSCOPIC FEATURES
General Features
Usually well circumscribed but unencapsulated
Tan or white, homogeneous cut surface with areas of hemorrhage and necrosis
Tumors may be deeply pigmented due to heavy melanin deposition
Size
Several millimeters to > 5 cm in greatest diameter
MICROSCOPIC PATHOLOGY
Histologic Features
Epithelioid melanoma
Nests or islands of large epithelioid cells with abundant eosinophilic cytoplasm that may resemble carcinoma
Tumor cells contain enlarged nuclei with prominent nucleoli
Spindle cell melanoma
Nests or short fascicles of atypical spindle cells resembling sarcoma
Differential diagnosis includes sarcomatoid lung carcinoma, metastatic sarcomatoid renal cell carcinoma, and spindle cell sarcoma
Mixed spindle and epithelioid cell melanoma
Most common form of metastatic melanoma, showing admixture of both spindle and epithelioid cells
Can be confused for a variety of other primary and metastatic sarcomas in the lung
Pleomorphic melanoma
Characterized by sheets of pleomorphic and anaplastic tumor cells with bizarre nuclei and frequent abnormal mitoses
METASTATIC MALIGNANT MELANOMA
Tumors may resemble pleomorphic high-grade sarcoma (MFH) or pleomorphic/anaplastic carcinoma of lung
“Rhabdoid” melanoma
Composed of sheets of large tumor cells with eccentric, densely eosinophilic cytoplasmic inclusions
Tumor cells can resemble rhabdomyoblastic cells in rhabdomyosarcoma or in “malignant rhabdoid tumor”
Signet ring cell melanoma
Sheets of tumor cells characterized by signet ring cell morphology
Cells will show enlarged, hyperchromatic nuclei displaced to periphery by abundant cytoplasm
Small cell melanoma
Dense sheets of monotonous small round tumor cells with hyperchromatic nuclei and scant cytoplasm
Tumors can resemble malignant lymphoma, carcinoid tumors, and other small round blue cell tumors
Cytologic Features
Hallmark of malignant melanoma is presence of cells with marked cytologic atypia
Majority of tumor cells are large, pleomorphic, with enlarged nuclei and prominent eosinophilic nucleoli
Frequent mitotic figures; abnormal mitoses are often encountered
Cells may also be small and relatively bland-appearing with minimal cytologic atypia
ANCILLARY TESTS
Immunohistochemistry
S100 protein is positive in nearly 100% of cases (nuclear and cytoplasmic stain)
In most cases, melanocytic-associated markers are positive: HMB-45, Melan-A, tyrosinase, microphthalmia transcription factor (MiTF)
Aberrant expression of epithelial markers (keratins, CEA, EMA) can be seen in small percentage of cases
Other markers can also be expressed, including CD10, CD56, CD68, CD99, CD117, calretinin, NSE, vimentin, and Bcl-2, but are nonspecific
DIFFERENTIAL DIAGNOSIS
Sarcomatoid Carcinoma
Tumor cells are positive for epithelial markers (cytokeratin, EMA, MOC31) and negative for S100 and melanocytic markers
Metastatic Renal Cell Carcinoma
Can show similar morphology with nests of tumor cells with abundant eosinophilic or granular cytoplasm
Tumor cells are positive for cytokeratin, EMA, and RCC marker, and negative for melanoma-associated markers and S100
Spindle and Epithelioid Cell Sarcomas
Tumors such as leiomyosarcoma, epithelioid sarcoma, and synovial sarcoma may resemble melanoma morphologically
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


