Mediastinal Teratoma
Key Facts
Etiology/Pathogenesis
Some authors have proposed the possibility of ectopically misplaced germ cells
Clinical Issues
Incidence
Most common germ cell tumors in anterior mediastinum
Approximately 45% of all mediastinal germ cell tumors
More common in young individuals
Most common germ cell tumor in children
May be more common in males (approximately 2:1)
Teratomas with malignant component may be more common in males
Symptoms
Precocious puberty
Hematologic conditions
Chest pain
Dyspnea
Asymptomatic
Macroscopic Features
Cyst and solid tumors
Presence of hair or teeth
Presence of sebaceous material
Microscopic Pathology
Mature elements derived from 3 germ cell layers
Mature teratoma
Immature teratoma
Teratomas with malignant component
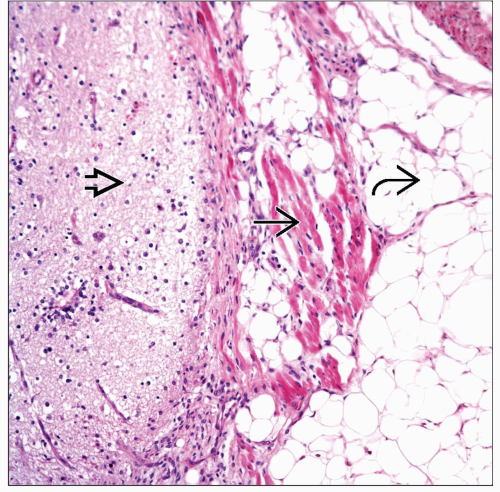 Mediastinal teratoma shows mature glial tissue  adjacent to fibers of skeletal muscle adjacent to fibers of skeletal muscle  and mature adipose tissue and mature adipose tissue  . Note that all tissues are mature. . Note that all tissues are mature. |
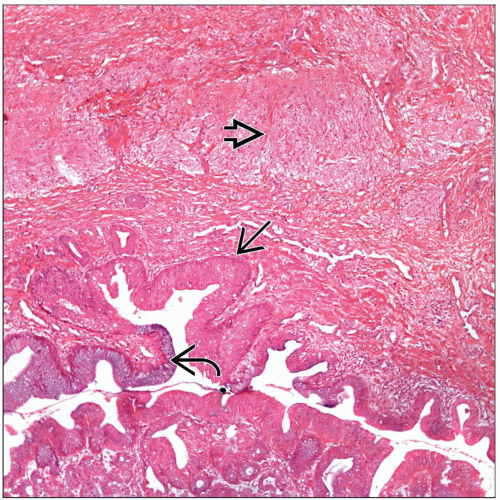 Mediastinal mature teratoma is shown with presence of cystic structures lined by squamous  and glandular epithelium and glandular epithelium  . Mature glial tissue is also present . Mature glial tissue is also present  . . |
TERMINOLOGY
Definitions
Neoplasm showing tissues derived from 3 germinal layers
At least 2 must be present
ETIOLOGY/PATHOGENESIS
Etiology
Although an unequivocal explanation for the occurrence of mediastinal germ cell tumors is not available, some authors have proposed the possibility of ectopically misplaced germ cells
CLINICAL ISSUES
Epidemiology
Incidence
Most common germ cell tumors in anterior mediastinum
Approximately 45% of all mediastinal germ cell tumors
Age
More common in young individuals
Teratomas are most common germ cell tumor in children
Gender
Mature teratomas may be more common in males (approximately 2:1)
Teratomas with malignant component may be more common in males
Site
Teratomas more common in anterior mediastinum
Posterior mediastinum may be site in unusual cases
Presentation
Cough
Chest pain
Dyspnea
Hemoptysis
Klinefelter syndrome
Hematologic conditions
Precocious puberty
Asymptomatic
Treatment
Surgical approaches
Mature teratomas: Complete surgical resection
Immature teratomas: Chemotherapy may be used
Teratomas with another malignant component: Chemotherapy
Prognosis
Mature teratomas: Prognosis is good in majority of cases
Immature teratomas: Depends on clinical stage
Teratomas with another malignant component: Clinical stage and type and percentage of malignant component are important parameters to determine prognosis
IMAGE FINDINGS
General Features
Calcification in 20-40% of cases
Fat-fluid levels are considered classic for teratomas
MACROSCOPIC FEATURES
General Features
Cyst and solid tumors
Presence of hair or teeth
Presence of sebaceous material
Sections to Be Submitted
Size
Vary in size from a few cm to > 15 cm in diameter
MICROSCOPIC PATHOLOGY
Histologic Features
Mature teratoma
Mature elements derived from 3 germ cell layers
Pancreatic tissue is commonly seen
Presence of skin adnexa is commonly seen
Immature teratoma
Presence of neural tubules
Presence of rosettes
Teratomas with malignant component
Seminoma
Yolk sac tumor
Embryonal carcinoma
Choriocarcinoma
Another malignant epithelial component: Adenocarcinoma, etc.
Presence of malignant mesenchymal component
Angiosarcoma
Rhabdomyosarcoma
Osteosarcoma
Chondrosarcoma
Predominant Pattern/Injury Type
Biphasic
Predominant Cell/Compartment Type
Germ, nonseminomatous
DIFFERENTIAL DIAGNOSIS
Sarcoma
Pure malignant mesenchymal neoplasms (sarcomas) do not show other type of epithelial differentiation
Carcinoma
Strictly malignant epithelial tumors; do not show other germinal layer components
Other Germ Cell Tumor
Presence of at least 2 different germ cell layers is diagnostic of teratoma
DIAGNOSTIC CHECKLIST
Clinically Relevant Pathologic Features
Gross appearance
Pathologic Interpretation Pearls
Presence of following features should help in diagnosis
Tissues from different germ cell layers
Neural tubules &/or rosettes
Malignant mesenchymal components
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


