Malignant Mesothelioma
Key Facts
Etiology/Pathogenesis
Mesotheliomas have been linked closely to asbestos exposure
Clinical Issues
Rare tumor that accounts for approximately 4-7 cases per 1,000,000 individuals
Tumor is more common in 5th & 6th decades of life
Weight loss
Chest pain
General malaise
Extrapulmonary pneumonectomy
Decortication
More common in men
Microscopic Pathology
Tubulo-papillary
Sarcomatoid
Biphasic
Clear cell
Deciduoid
Adenomatoid
Glandular
Mucohyaline
Cartilaginous and osseous metaplasia
Desmoplastic
Lymphohistiocytic
Top Differential Diagnoses
Adenocarcinoma
Sarcoma
Synovial sarcoma
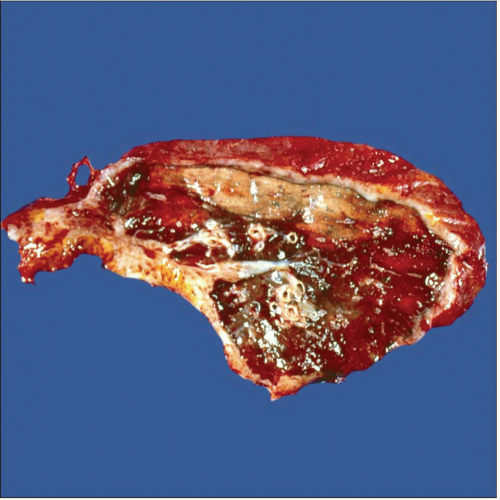 Extrapulmonary pneumonectomy consisting of both visceral and parietal pleuras, lung, and portions of diaphragm and pericardium is shown. Note the marked pleural thickening. |
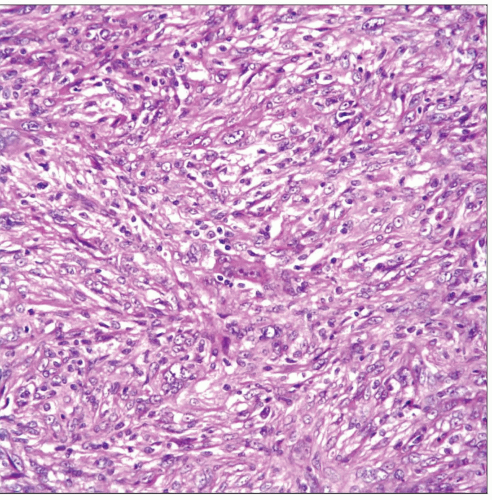 Sarcomatoid malignant mesothelioma shows a spindle cell proliferation closely mimicking the features of a mesenchymal neoplasm. |
TERMINOLOGY
Synonyms
Epithelioma
Term used in older literature
Definitions
Malignant neoplasm arising in serosal surfaces
ETIOLOGY/PATHOGENESIS
Environmental Exposure
Mesotheliomas have been linked closely to asbestos exposure
Other Possible Etiologies
Viral infection SV40
De novo
CLINICAL ISSUES
Epidemiology
Incidence
Rare tumor that accounts for approximately 4-7 cases per 1,000,000 individuals
Age
More common in 5th and 6th decades of life
Gender
More common in men
Presentation
Weight loss
Chest pain
Cough
Shortness of breath
Pleural effusion
Treatment
Surgical approaches
Extrapulmonary pneumonectomy
Decortication
Pleural peeling
Adjuvant therapy
Chemotherapy
Prognosis
Poor
12-18 month average survival
MACROSCOPIC FEATURES
General Features
Diffuse thickening of pleura
In rare cases, tumor will present as localized pleural-based tumor
MICROSCOPIC PATHOLOGY
Histologic Features
Homogeneous cellular proliferation without much mitotic activity or cellular pleomorphism
Predominant Pattern/Injury Type
Tubulo-papillary
Sarcomatoid
Biphasic
Predominant Cell/Compartment Type
Epithelial
Spindle
Other Growth Patterns
Clear cell
This pattern is characterized by presence of cellular proliferation in which cells show clear cytoplasm
Low mitotic count
Most of these tumors do not show extensive areas of necrosis
Deciduoid
This pattern is composed of medium-sized cells with excentric nuclei and inconspicuous nucleoli
Low mitotic count
Necrosis and prominent nuclear atypia are not common
Adenomatoid
Cords of neoplastic cells forming cystic spaces
Signet ring cell-like
Low mitotic count
Areas of necrosis or hemorrhage are not common
Glandular
Prominent glandular component
Glands of different sizes
Most closely mimics adenocarcinoma
Mucohyaline
Extensive pools of mucoid material
Neoplastic cells embedded or floating in pools of mucoid material
Cartilaginous and osseous metaplasia
Very unusual growth pattern
Tumor shows extensive areas of cartilaginous or osseous differentiation
Numerous osteoclast giant cells
Desmoplastic
Low cellularity
Easily mistaken for a benign tumor
Neoplastic cells, either spindle or oval, dissecting fibrocollagen
Areas of necrosis are not readily apparent
Lymphohistiocytic
Mixture of epithelioid cells, lymphocytes, and histiocytes
May mimic thymoma or lymphoma
ANCILLARY TESTS
Electron Microscopy
Transmission
Elongated microvilli
Well-developed cell junctions
DIFFERENTIAL DIAGNOSIS
Metastatic Adenocarcinoma
Shows positive staining for carcinomatous epitopes, including CEA, MOC31, and BER-EP4
History of primary tumor elsewhere is important
Sarcoma
Sarcomas encasing lung parenchyma are rather unusual
It would be unusual for mesothelioma to stain with mesenchymal markers other than vimentin
Clinical history is important to rule out a metastasis
Synovial Sarcoma
Either mono- or biphasic tumors may mimic mesothelioma
Monophasic tumors will show positive staining for Bcl-2, which would be unusual in mesothelioma
Synovial sarcoma shows characteristic X;18 translocation
Thymoma
In cases of lymphohistiocytic mesothelioma
Use of immunohistochemical studies show strong p63(+) in thymoma
Although thymomas may occur as pleural tumors, they are more common in anterior mediastinum
Metastatic Clear Cell Carcinoma
In cases of clear cell mesothelioma
Use of immunohistochemical studies will lead to correct interpretation
Metastatic Osteogenic Sarcoma
In cases of mesothelioma with osseous and cartilaginous components
Clinical history of previous osteosarcoma will be necessary for correct diagnosis
DIAGNOSTIC CHECKLIST
Clinically Relevant Pathologic Features
Invasive pattern
Penetration of tumor cells into fat
SELECTED REFERENCES
1. Arrossi AV et al: Histologic assessment and prognostic factors of malignant pleural mesothelioma treated with extrapleural pneumonectomy. Am J Clin Pathol. 130(5):754-64, 2008
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


