Lymphoid Effusions and Lymphomas
Donna M. Coffey, MD
Norma Quintanilla, MD
Key Facts
Clinical Issues
TB is most common cause of pleural effusion in developing countries
TB effusions have small mature T lymphocytes
10-15% of malignant effusions are caused by lymphomas and most cases represent secondary involvement of serosal surfaces
˜ 8% of patients present with no prior diagnosis of lymphoma
Effusions due to lymphomas reduce overall survival and predict disease relapse after chemotherapy
Cytopathology
Exact subtyping requires correlation of cytomorphology with clinical findings and ancillary studies, such as immunocytochemistry, flow cytometry, and cytogenetics/molecular testing
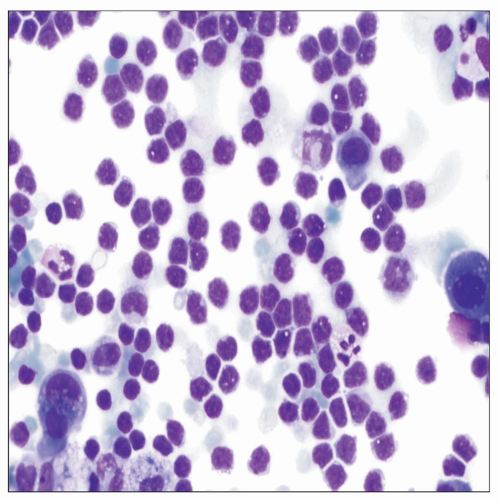 Diff-Quik shows pleural fluid with CLL characterized by a uniform population of small mature lymphocytes with scant cytoplasm and clumped chromatin. Differential diagnosis includes benign lymphoid-rich effusions. |
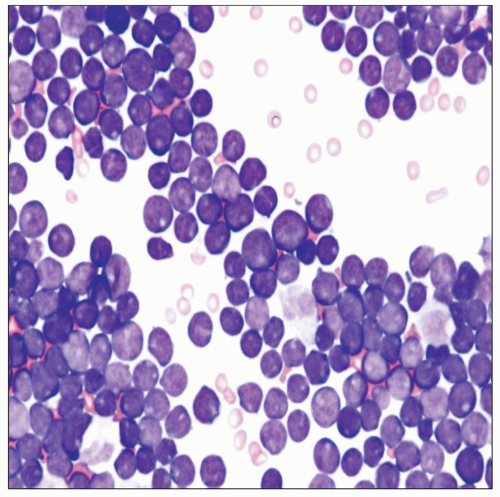 Diff-Quik-stained cytospin of pleural effusion in a case of T-lymphoblastic leukemia/lymphoma demonstrates cells with high N:C ratio, fine chromatin, and scant cytoplasm. |
CLINICAL ISSUES
Presentation
Benign lymphoid-rich effusions can be seen in patients with tuberculosis (TB) and status post coronary artery bypass
TB is the most common cause of pleural effusion in developing countries
Lymphoid-rich effusions contain small mature T lymphocytes
In adult patients, 10-15% of malignant effusions are caused by lymphomas
Most represent secondary involvement of serosal surfaces as part of disseminated disease
Lymphoma/leukemia effusions are more common in pediatric population
Hodgkin disease (HD) effusions are caused by mediastinal lymphadenopathy or thoracic duct obstruction
Non-Hodgkin lymphoma (NHL) effusions are caused by direct pleural/pulmonary involvement
˜ 20-30% of malignant pleural effusions are caused by NHL or HD
Pericardial and peritoneal cavity involvement is less common
Primary effusion lymphomas (PEL) are high-grade B-cell lymphomas that involve serous cavities without detectable solid tumor mass
Patients with NHL pleural effusions present with shortness of breath, mediastinal tumors, lymphadenopathy, and extranodal solid tumors
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


