Lymph Nodes Below Diaphragm: Diagnosis
 Metastatic carcinomas should closely resemble the primary carcinoma. This abdominal lymph node shows both metastatic well-differentiated colon carcinoma  and prostate carcinoma and prostate carcinoma  . . |
 Benign inclusions should be considered when epithelioid cells in nodes do not resemble a known primary carcinoma. Endosalpingiosis  , decidual reaction, and mesothelial cells should be considered. , decidual reaction, and mesothelial cells should be considered. |
SURGICAL/CLINICAL CONSIDERATIONS
Goal of Consultation
Evaluate peritoneal or inguinal lymph nodes for staging of a known carcinoma or to evaluate lymphadenopathy
Change in Patient Management
Planned surgical procedure for curative intent may be modified or canceled if metastatic carcinoma is found
Clinical Setting
Enlarged nodes may be detected during surgery for a benign condition
If malignant, additional surgical exploration and biopsies may be performed to detect primary carcinoma
Nodes are routinely sampled for staging of known carcinomas of abdominal cavity prior to definitive surgery
For some carcinomas, surgical approach will be altered if metastatic carcinoma is detected
For other carcinomas, surgical treatment is indicated even if metastatic carcinoma is present
SPECIMEN EVALUATION
Gross
Specimen usually consists of excision of a nodule presumed grossly to be a lymph node
If surrounded by adipose tissue, nodule should be separated by palpation and dissection
Size and contours (e.g., smooth or irregular) of nodule are recorded
Nodule is serially sectioned
Focal firm white areas are typical of metastatic carcinoma
Diffusely enlarged node with fleshy surface is most likely lymphoma
Hard, difficult to cut nodule is most likely an infarcted epiploic appendage
Mottled nodes with focal necrosis may be involved by infectious process
Frozen Section
If patient has known carcinoma and biopsy is performed for staging prior to performing surgery, it is preferable to submit entire node for frozen section
If only a portion of node is frozen, a small metastasis can be missed
If patient does not have known carcinoma, specimen should be sampled such that diagnosis will be possible on permanent sections &/or with ancillary studies
Nonfrozen tissue for ancillary studies may be helpful
Cytologic preparations are preferred if infection or lymphoma are suspected
If cytologic preparations do not provide diagnosis, portion of node may be frozen
Cytology
Scrape or touch preparations can be made from cut surface(s) of node
MOST COMMON DIAGNOSES
Metastatic Carcinoma
Almost always resemble primary carcinoma
Location and histologic type of known or suspected primary carcinoma is essential information
Seminoma can be associated with granulomas
If suspected metastasis does not resemble primary, consider other diagnoses
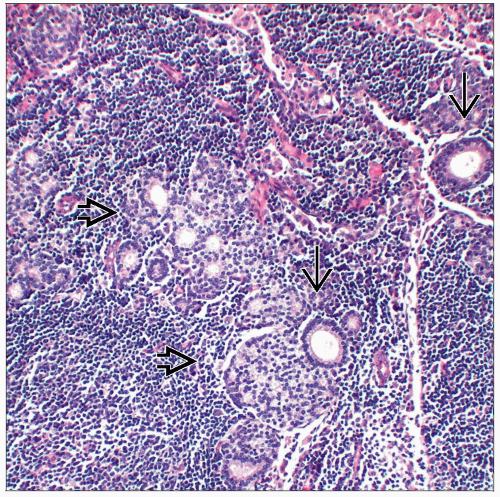
Endosalpingiosis (Müllerian Inclusions)
In women, benign tubular epithelium can be found in lymph nodes
May be associated with psammoma body calcifications
Very rarely present in males
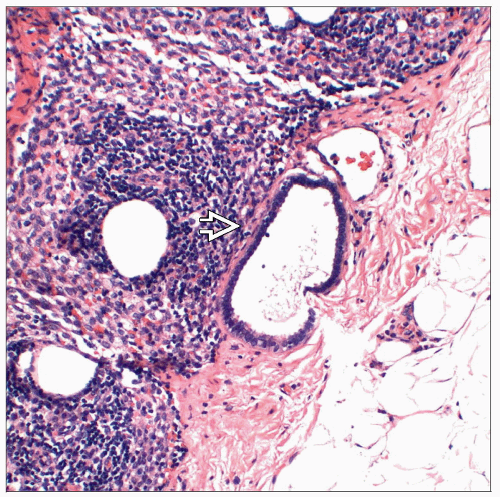
Tubules are lined by single layer of low cuboidal cells
Nuclei are small with inconspicuous nuclei
Cilia may be present
Squamous metaplasia can occur
Final classification may require immunohistochemical studies
Ectopic Decidua
Stromal tissue, under influence of progesterone during pregnancy, can undergo decidual changes
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


