Lung: Nonneoplastic Diffuse Disease: Diagnosis
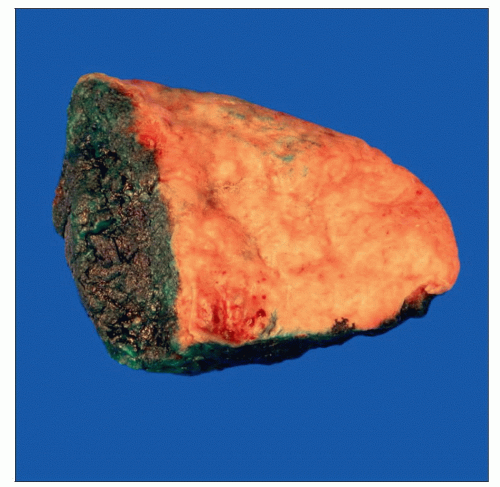 Tissue procured to diagnose nonneoplastic lung disease is generally taken as a wedge-shaped fragment from the periphery of 1 or multiple lobes. Staples in the margin, if present, must be removed. |
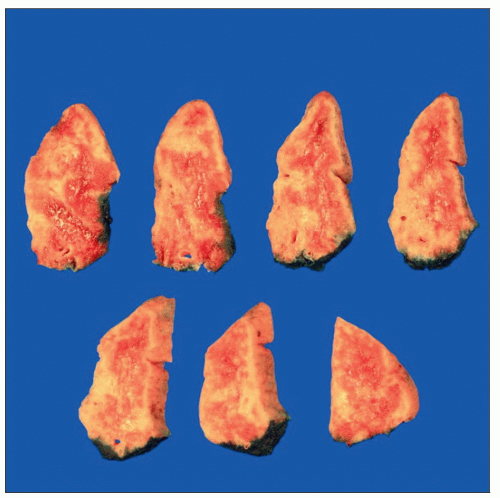 The wedge biopsy is serially sectioned in parallel to the long axis of the specimen and examined for any focal lesions. A representative section may be submitted for frozen section evaluation. |
SURGICAL/CLINICAL CONSIDERATIONS
Goal of Consultation
Provide preliminary diagnosis for patients with diffuse lung disease and aid in allocation of tissue for special studies
Change in Patient Management
Preliminary diagnosis can help guide immediate management (inflammatory vs. infection vs. neoplasm)
Clinical Setting
Majority of patients are critically ill; clinical differential diagnosis includes a variety of neoplastic, infectious, or inflammatory causes
SPECIMEN EVALUATION
Gross
Specimen is serially sectioned and examined thoroughly to exclude any focal or mass lesions
Specimen is kept sterile in case tissue needs to be taken for cultures or other special studies (1 cm3 is minimal amount of tissue for testing)
Frozen Section
Representative section of tissue is frozen
MOST COMMON DIAGNOSES
Bronchopneumonia/Abscess
Tissue may need to be taken for culture if not already done so clinically
Granulomatous Inflammation
Necrotizing granulomas favor infection, and diagnostic findings (e.g., fungal yeast or hyphae) should be mentioned, if present
Numerous confluent, well-formed, nonnecrotizing granulomas in lymphangitic distribution suggest sarcoidosis
Rare, poorly formed interstitial granulomas or histiocyte aggregates may suggest hypersensitivity pneumonitis
Confluent (geographic) zones of necrosis with scattered multinucleated giant cells and without wellformed granulomas may suggest granulomatosis with polyangiitis (previously Wegener granulomatosis)
Viral Infection
Must demonstrate viral inclusions, often in a background of necrotizing pneumonitis or diffuse alveolar damage
Prominent nucleoli in reactive pneumocytes can mimic inclusions but lack a peripheral halo
Interstitial Lung Disease
If interstitial lung disease is suspected on frozen section, final diagnosis should be deferred to permanent sections for thorough sampling
REPORTING
Frozen Section
Description of histologic findings is generally sufficient (e.g., nonnecrotizing granulomatous inflammation, patchy interstitial fibrosis)
Absence of neoplasm should be noted
Most nonneoplastic entities will require evaluation of permanent sections, thus a final diagnosis is often deferred
PITFALLS
Failure to Identify a Malignant Process
Dense inflammatory infiltrates can obscure malignant cells
RELATED REFERENCES
1. Sienko A et al: Frozen section of lung specimens. Arch Pathol Lab Med. 129(12):1602-9, 2005
Image Gallery
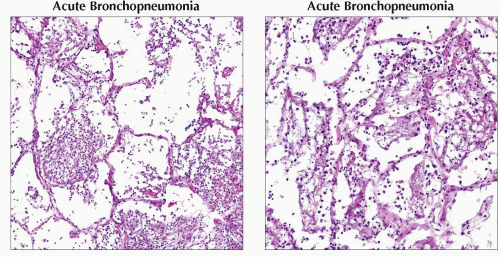 (Left) Acute bronchopneumonia is characterized by predominantly acute inflammatory cells (neutrophils) within the alveolar spaces &/or lumina of bronchioles. This finding can be diffuse, patchy, or somewhat focal. The infiltrate may also be associated with food particles in cases of aspiration pneumonia. (Right) The neutrophilic infiltrate may be associated with bacterial clusters, fungal elements, or food material, depending on the etiology. Tissue should always be sent for microbiologic culture. |
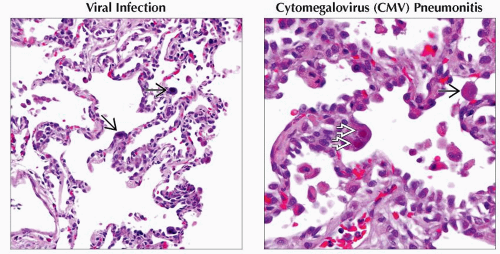 (Left) A diagnostic finding in certain viral infections is the presence of nuclear &/or cytoplasmic inclusions. These inclusions
 vary in size, but most have a dark-staining quality that allows for identification even at lower magnifications. The background lung may show necrosis, pneumonitis, or diffuse alveolar damage. (Right) This image shows 2 nuclear “owl’s-eye” inclusions vary in size, but most have a dark-staining quality that allows for identification even at lower magnifications. The background lung may show necrosis, pneumonitis, or diffuse alveolar damage. (Right) This image shows 2 nuclear “owl’s-eye” inclusions  and 1 eosinophilic granular cytoplasmic inclusion and 1 eosinophilic granular cytoplasmic inclusion  , characteristic of cytomegalovirus (CMV) infection. , characteristic of cytomegalovirus (CMV) infection.Stay updated, free articles. Join our Telegram channel
Full access? Get Clinical Tree
 Get Clinical Tree app for offline access
Get Clinical Tree app for offline access

|