Low Anterior Rectal Resection: Laparoscopic Technique
Joël Leroy Didier
Mutter Jacques Marescaux
DEFINITION
Low anterior resection (LAR) is the full mobilization and resection of the rectum at the level of the levators, leaving behind only a short or no rectal stump.
LAR for rectal cancer requires a total mesorectal excision (TME) to ensure a radical resection with adequate radial and distal margin. The goal is to achieve an en bloc resection of the cancer with complete dissection of the pararectal lymph nodes contained within the mesorectum.
Laparoscopic LAR is a minimally invasive approach to TME with significant short-term advantages when compared to open LAR, including less pain, faster recovery, lower morbidity, and shorter hospital stays, without compromising the oncologic safety of the operation.
PATIENT HISTORY AND PHYSICAL FINDINGS
A full history and physical examination will allow the surgeon to determine if a sphincter-sparing operation is possible, whether a temporary ileostomy is likely, and will also aid in discussions regarding postoperative functional status.
History elements elicited should include baseline functional status, bowel incontinence, sexual and urinary dysfunction, as well as pain with defecation or tenesmus. Previous history of pelvic radiation and pelvic surgery should also be noted.
History of incontinence should prompt discussions regarding postoperative quality of life with a low anastomosis.
History of pain or tenesmus suggests involvement of the anal sphincter or a larger tumor. This will alter the course of treatment and a sphincter-sparing operation may not be possible in this subgroup of patients.
Physical examination should include a digital rectal exam (DRE), vaginal exam, anoscopy, and a thorough abdominal exam.
DRE should assess tumor size, degree of fixation to rectal and pelvic wall, mobility, location (anterior/posterior/lateral), distance from the anorectal ring, and anterior extension into vagina/prostate. Anal sphincter involvement can also be determined by DRE in the majority of patients.
Anterior rectal tumors in female patients require a vaginal exam to rule out extension into the vagina.
Anoscopy for low rectal tumors may allow for better visualization of the tumor during the physical exam.
The abdominal exam should evaluate for liver metastasis. A bilateral groin exam should be performed to evaluate for potential inguinal lymphadenopathy.
IMAGING AND OTHER DIAGNOSTIC STUDIES
A colonoscopy with documentation of all polyps should be performed. Suspicious lesions should be tattooed to facilitate localization during surgery.
Staging with endorectal ultrasound or rectal magnetic resonance imaging (MRI) should be performed to determine the need for neoadjuvant therapy and to plan operative strategy. A computed tomography (CT) of the chest, abdomen, and pelvis evaluates for potential metastases.
A preoperative carcinoembryonic antigen level should be obtained.
SURGICAL MANAGEMENT
Preoperative Planning
Informed consent is obtained preoperatively. The patient has been informed of the potential necessity to perform a diverting ileostomy or end colostomy.
Potential ostomy sites are marked the evening before the intervention.
We follow the Society of American Gastrointestinal and Endoscopic Surgeons’ (SAGES) bowel preparation guidelines.
Appropriate intravenous antibiotics are administered within 1 hour of skin incision.
Equipment and Instrumentation
10-mm, 0-degree camera (30-degree camera is optional) with high-resolution monitors
Laparoscopic endoscopic scissors and a blunt tip, 5-mm energy device (10-mm can be useful in obese patients)
Laparoscopic linear staplers
Positioning and Port Placement
Patient setup
Patient setup is a major operative step.
The patient should be adequately secured to the table.
Adequate padding is essential to prevent nerve and venous compressions.
The patient is placed in a supine position with a cushion placed underneath the left flank in order to obtain a moderate lateral decubitus, which will retract bowel loops toward the right part of the abdomen.
A rotation to the right and a caudal head tilt (Trendelenburg position) will help to retract bowel loops by means of gravity.
The patient’s legs will then be spread apart in a semiflexion using adjustable leg supports to allow for a double abdominal and perineal access.
One should control the perfect positioning of the buttocks at the distal edge of the table to allow for an easy access to the anal and perineal area.
The arms are padded and tucked.
An orogastric tube is inserted; it will be removed at the completion of the surgery.
A Foley catheter is inserted; it will be left in place for 24 hours.
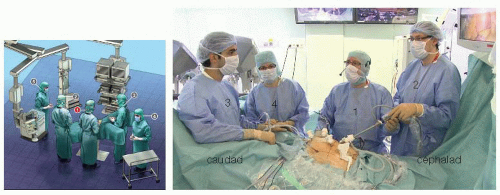 FIG 1 • Team setup. Surgeon (1). First assistant (2). Second assistant (3). Scrub nurse (4). Anesthesiologist (5). |
Team positioning
This procedure is performed with two assistants and a scrub technician.
During the abdominal part of the procedure (FIG 1), the surgeon stands on the right flank of the patient, his or her first assistant lateral to the patient’s right shoulder, and the second assistant in between the patient’s legs. The scrub technician is then located to the right of the surgeon lateral to lower limbs.
During the perineal part of the procedure, the entire team shifts toward the extremity of the table once the perineum has been exposed.
The monitors are placed in front of the operating team and at eye level to improve ergonomics.
Port placement
One 12-mm supraumbilical port (port A) is introduced first using a mini-open technique. It will be used to accommodate the camera (FIG 2).
Two other ports, a 5-mm port in the right flank (port B) and a 12-mm port in the right iliac fossa (port C), are used as operating ports (FIG 2).
The fourth port in the left flank at the level of the umbilicus is inserted through the rectus muscle (port D, 5 mm in diameter), where the colostomy will be performed (FIG 2).
The last port introduced in the suprapubic area (port E, 12 mm in diameter) is used for pelvic retraction and for exposure of the sigmoid colon’s root (FIG 2).
Port fixation in the wall should be perfect in order to prevent any risk of parietal injury and to prevent increased operative times due to a loss in abdominal pressure. One should not hesitate to fix ports to the skin.
Additional ports may be used in case of difficulty in exposure. In this case, a port will be positioned in the right hypochondrium (port F) to retract the ileocecal area. This is particularly useful in obese patients (FIG 2).
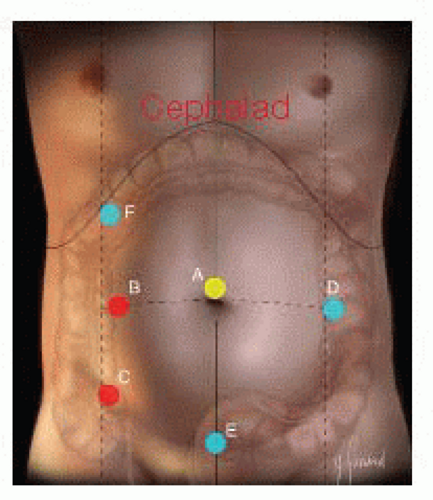 FIG 2 • Port placement. Optical port (A). Working ports (B,C). Retracting ports (D,E). Additional retracting port (F). |
TECHNIQUES
LAPAROSCOPIC LOW ANTERIOR RESECTION
Exploration and Exposure
The intervention is begun by an exploration of the abdominal cavity to locate the tumor and evaluate for possible metastases. It also allows to expose the pelvis and to evaluate the length and quality of the sigmoid loop, which will allow determining the type of mobilization of the left colon and of the splenic flexure.
The tumor’s identification may be necessary and especially so for tumors located proximally. Combined endoscopy may be required in cases where an effective preoperative marking could not be performed on the day before the intervention.
Exposure is improved by placing the patient in a Trendelenburg position with the table tilted to the right.
In women, exposure of the posterior pelvis and of the rectovaginal (Douglas’) pouch can be obtained by direct or indirect suspension of the uterus by means of the T’Lift™ (VECTEC, France) tissue retraction device (FIG 3A,B) or suprapubic transparietal sutures (FIG 4A,B).
Visceral obesity (in male patients) is more incapacitating than subcutaneous obesity (in female patients). The use of retractors is very helpful.
Primary Vascular Oncologic Approach to the Sigmoid Colon
As for any oncologic surgical procedure, a primary vascular approach is the rule.
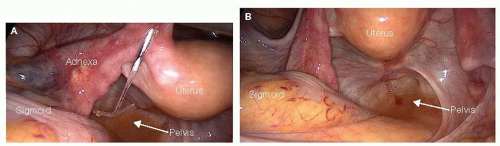
FIG 3 • T’Lift™ tissue retraction system. A. T’Lift™ tissue retraction system passed through the round ligament. B. Pelvic exposure in women after bilateral uterine suspension with T’Lift™ tissue retraction system.
In rectosigmoid cancer, one should approach the inferior mesenteric vessels at their origin in order to perform an “en bloc” removal of all lymph nodes associated with the rectosigmoid junction (D3 resection). It does not preclude the potential preservation of the proximal inferior mesenteric artery (IMA) and of the left colic artery (LCA).
We always start with a primary approach to the IMA. The inferior mesenteric vein (IMV) is then approached in order to prevent any venous overload related to the late ligation of the IMA.
Once the root of the sigmoid mesocolon has been exposed, the left retroperitoneal space is opened by incising the posterior peritoneum from the anterior aspect of the promontory up to the left border of the duodenojejunal junction (ligament of Treitz) (FIG 5A).
Once the retroperitoneum has been opened, dissection is initiated opposite the promontory on the posterior aspect of the inferior mesenteric vascular sheath (i.e., the superior rectal artery at this level). This step is facilitated by the anterior traction on the mesocolon, which induces the pneumodissection of the retrovascular space, thanks to intraabdominal carbon dioxide pressure.
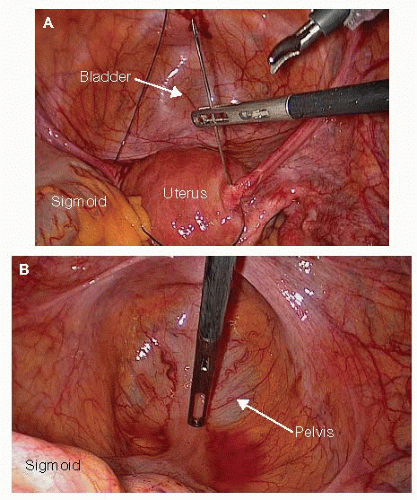
FIG 4 • A. Transparietal suprapubic sutures for uterine suspension. B. Exposure of the pelvis in women after transparietal suprapubic suture uterine suspension.
Dissection is carried on in contact with the vascular sheath cranially until the origin of the IMA on the aorta.
The dissection is continued from caudad to cephalad in contact with the artery, which is skeletonized over approximately 2 cm in order to achieve ligation and division 1 or 2 cm away from the aorta (FIG 5B).
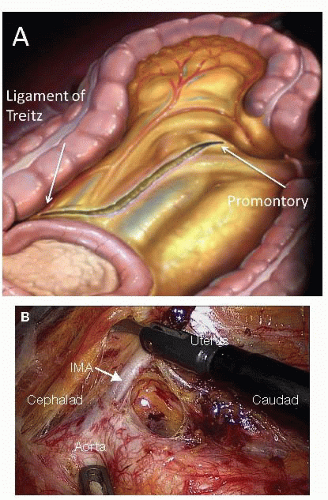
FIG 5 • Dissection of the IMA. A. Opening of the left retroperitoneal space by incising the posterior peritoneum from the anterior aspect of the promontory to the ligament of Treitz. B. The IMA has been dissected 1 to 2 cm from the aorta.
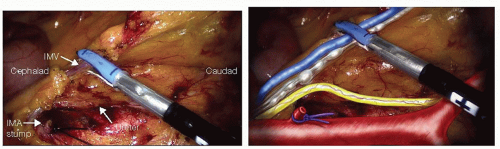
FIG 6 • IMV transection at the level of the ligament of Treitz. The IMA was previously transected off the aorta. The retroperitoneal structures are exposed.
This technique allows preserving sympathetic nerve plexuses, which course along the aorta on its right anterior aspect.
Division of the IMA is performed with the LigaSure™ vessel-sealing device using a ligation with a loop on the IMA stump.
Once the IMA has been divided, the assistant standing between the patient’s legs will grasp the artery using an atraumatic forceps introduced into the suprapubic port (port D) and apply anterior traction to ideally expose dissection planes in contact with the left posterior and lateral aspects of the artery.
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


