Liver, Intrahepatic Mass: Diagnosis and Margins
 Oligometastatic colon carcinoma or neuroendocrine tumors to the liver may undergo resection. Surgeons often request intraoperative evaluation of the hepatic margin to ensure complete resection. |
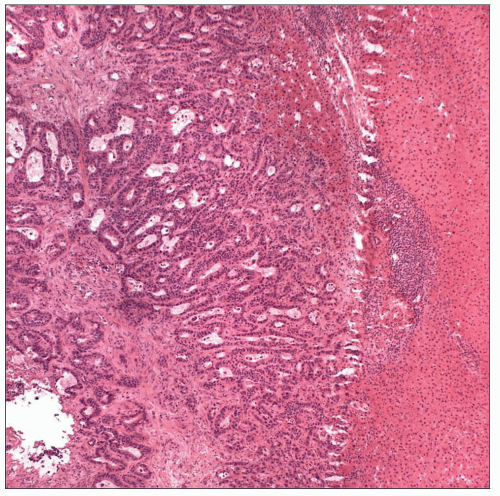 Metastatic colon carcinoma is usually easily recognized by columnar cells and dirty necrosis. If the lesion is a small nodule on the liver capsule, bile duct adenoma or hamartoma should be considered. |
SURGICAL/CLINICAL CONSIDERATIONS
Goal of Consultation
Determine whether liver mass is benign or malignant
Evaluation of margins
Change in Patient Management
If lesion is benign, wide margin of resection is unnecessary
If lesion is present at margin, additional tissue is removed, if surgically feasible
Clinical Setting
Liver lesions will usually have been diagnosed by core needle biopsy or fine-needle aspiration prior to surgery
Open biopsy may be preferred in some cases due to concern for needle-track seeding
Patients may benefit from resection of
Hepatocellular adenoma
Focal nodular hyperplasia, increasing in size or multiple
Hepatocellular carcinoma
Intrahepatic cholangiocarcinoma
Oligometastatic carcinoma to liver (colon cancer most common primary site)
Metastatic neuroendocrine tumors
Malignant lesions are resected with a margin of at least 1 cm, if possible
Superficial or capsular liver mass may be detected during operation for another reason
Surgeon may request intraoperative evaluation to guide surgery and for staging
SPECIMEN EVALUATION
Gross
Measure specimen in 3 dimensions
Cut parenchymal portion of liver is identified
Evaluate surface for any areas grossly suspicious for tumor involvement
Ink margin
Liver capsule is not a margin and should not be inked
Be wary of ink leaking into cracks in tissue
Thinly slice specimen perpendicular to margin
Identify all mass lesions
Number of metastatic foci found in resection has clinical and prognostic relevance
Correlation with number of lesions seen on imaging is necessary to ensure surgeon removed all foci of tumor
Slices must be 4-5 mm thick to detect small metastatic foci
Measure closest distance to margin
Only a fibrotic tumor bed may be visible in posttreatment resections
Frozen Section
If there is a grossly suspicious area for margin involvement, perpendicular frozen section should be evaluated
MOST COMMON DIAGNOSES
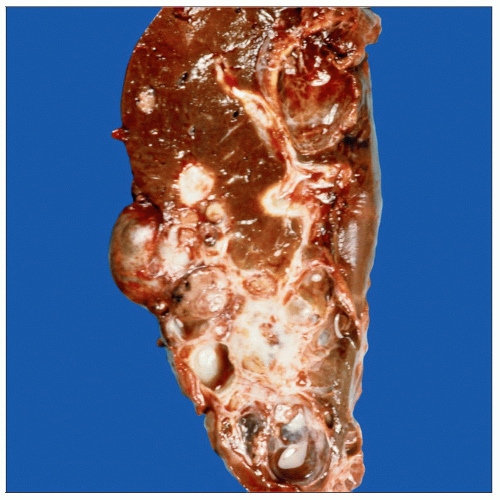
Metastatic Carcinoma
Most common diagnosis (˜ 25% of total, ˜ 75% of malignant diagnoses)
Multiple hard white masses
Often with central necrosis
Oligometastatic colonic carcinoma may be resected
Margin should be free of carcinoma but wide margin is not required
Hepatocellular Carcinoma
2nd most common diagnosis (˜ 25% of malignant diagnoses)
May present as a solitary mass, dominant mass with satellite nodules, or rarely, in diffusely infiltrative pattern
Variegated yellow-white appearance with necrosis and hemorrhage in larger lesions
Surrounding liver is usually cirrhotic
Nodule within a nodule may be an area of carcinoma with a dominant nodule or carcinoma arising in a dysplastic nodule
Tumor cells closely resemble normal hepatocytes when well differentiated
Large polygonal cells with large nucleus, prominent nucleolus, and abundant cytoplasm
Cytoplasmic bile may be present and support origin in liver
Thickened trabeculae with > 2 cells
Absent portal tracts
Poorly differentiated carcinomas are more easily recognized as malignant, but distinction of hepatocellular from cholangiocarcinoma may be difficult
Fibrolamellar carcinoma
Forms large (typically > 10 cm), circumscribed, hard brown mass
Surrounding liver is typically noncirrhotic
Cholangiocarcinoma
Most cancers are advanced at time of diagnosis
Large, gray-white, hard, irregular masses
Cholangiocarcinoma cannot be distinguished from metastatic adenocarcinoma on frozen section
Intrahepatic duct and bile duct margins should be evaluated for dysplasia and malignancy
Pediatric Tumors
Rare
Tissue for ancillary studies should be considered (electron microscopy, cytogenetic studies, snap frozen for molecular studies)
Some tumors that occur in adults also occur in children
Hepatocellular carcinoma
Focal nodular hyperplasia
Hepatocellular adenoma
Carcinomas may have undergone neoadjuvant therapy with chemotherapy &/or radiation
Hepatoblastoma
Large circumscribed mass with variegated appearance including cysts, necrosis, and hemorrhage
Mesenchymal hamartoma
Large circumscribed mass with multiple cystic spaces filled with fluid
Solid areas may fibrotic, myxoid, with entrapped foci of normal liver
Embryonal (undifferentiated) sarcoma
Usually occurs between ages of 6 and 11
Circumscribed soft tumor with solid and cystic appearance
Hemorrhage and necrosis may be present
Bile Duct Adenoma/Hamartoma
Form small (< 1 cm) to large (up to 4 cm) white circumscribed nodules on liver capsule
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


