Leiomyosarcoma
Bruce M. Wenig, MD
Key Facts
Terminology
LMS: Malignant tumor of smooth muscle
Etiology/Pathogenesis
May develop following irradiation or cyclophosphamide exposure
Appears to arise from vascular structures
Link between LMS and Epstein-Barr virus (EBV) identified
Occurs in immunocompromised patients
Clinical Issues
Approximately 4% arise in head and neck
Increased incidence in immunocompromised patients
Microscopic Pathology
Interlacing fascicular to storiform bundles of spindle-shaped cells
Typically intersect at right angles
Neoplastic cells are elongated (spindle) with centrally located, blunt-ended, cigar-shaped nuclei and eosinophilic cytoplasm
Perinuclear vacuole or clear halo may be seen, giving nucleus an indented or concave contour
Variable degree of cellular anaplasia with nuclear pleomorphism, nuclear hyperchromasia, and increased mitotic activity (typical and atypical forms)
Actins (smooth muscle and muscle specific) positive
Criteria for malignancy
Tumors with 1-4 mitoses per 10 HPF considered potentially malignant especially in conjunction with nuclear atypia and necrosis
> 4 mitoses per 10 HPF is malignant
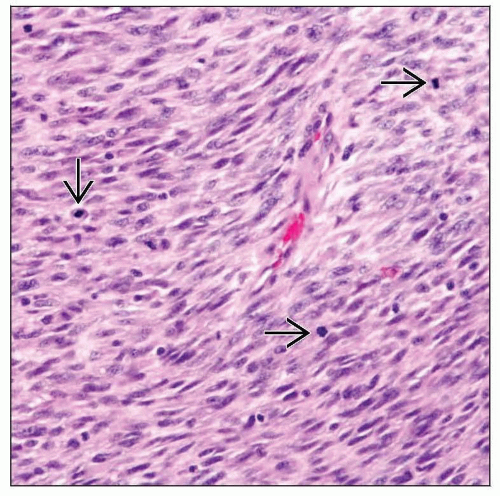 Sinonasal spindle-shaped cellular proliferation is shown with nuclear pleomorphism and increased mitotic activity  . The overall mitotic count was ≥ 4 mitoses per 10 high-power fields. . The overall mitotic count was ≥ 4 mitoses per 10 high-power fields. |
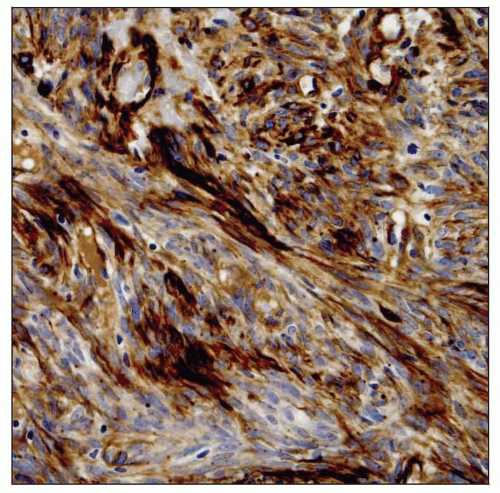 The presence of smooth muscle actin staining supports the light microscopic features in leiomyosarcoma (LMS). As head and neck LMS is rare, differentiation is required from other spindle cell neoplasms. |
TERMINOLOGY
Abbreviations
Leiomyosarcoma (LMS)
Definitions
Malignant tumor of smooth muscle
ETIOLOGY/PATHOGENESIS
Environmental Exposure
May develop following irradiation or cyclophosphamide exposure
Infectious Agents
Link between LMS and Epstein-Barr virus (EBV) identified
Occurs in immunocompromised patients
Histogenesis
Appears to arise from vascular structures
Due to relative lack of smooth muscle in head and neck region
Other than relationship to vascular walls, histology similar to non-vascular-derived LMS
CLINICAL ISSUES
Epidemiology
Incidence
Approximately 4% arise in head and neck
Increased incidence in immunocompromised patients
Post-transplantation (e.g., kidney, heart, liver)
AIDS
Epstein-Barr virus (EBV) found in these tumors, termed EBV smooth muscle tumors (EBVSMT)
Clonal EBV DNA and EBV surface receptor protein
Different episomal DNA clones found in separate tumors in same patient; suggests multifocal tumor rather than metastatic disease
Age
Non-immunocompromise-associated LMS
Occurs in wide age range
Most common in 6th decade
Immunocompromise-associated LMS
Tends to occur in children or young adults
Gender
Equal gender distribution
Site
Non-immunocompromise-associated LMS
Most common sites
Oral cavity (buccal mucosa, gingiva, tongue, floor of mouth)
Sinonasal tract
Skin and subcutaneous tissue
Less common sites
Larynx
Trachea
Neck
Hypopharynx
Orbit
External auditory canal
Immunocompromise-associated LMS
Tend to occur in relationship to viscera (e.g., GI tract, lung)
May be multifocal
Presentation
Nasal obstruction
Pain
Epistaxis
Painless mass
Ulceration
Treatment
Prognosis
Dependent on site and extent of tumor
Not necessarily contingent on histology
Nasal cavity
Good prognosis
Cured following complete removal
Both nasal cavity and paranasal sinuses
Aggressive neoplasm associated with increased recurrence (70% of patients)
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


