Laparoscopic Surgery of the Female Pelvis
This chapter provides an introduction to the laparoscopic anatomy of the female pelvis and uses several simple procedures to illustrate that anatomy. Obviously, a single chapter cannot do full justice to an entire subspecialty, but basic information about these procedures and the relevant laparoscopic anatomy will be useful to the general surgeon. References at the end give further technical details of more advanced procedures.
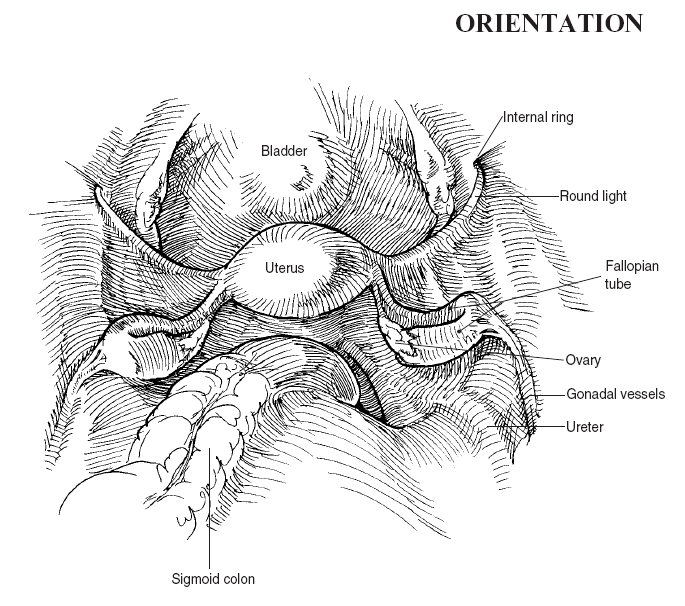
The laparoscopic view of the pelvis (see the orientation figure) is similar to that obtained with the uterus elevated and retracted for transabdominal hysterectomy (see also Fig. 85.2). The round ligaments arch up and laterally to exit through the internal (deep) inguinal rings. The uterus lies between bladder (anterior) and rectosigmoid colon (posterior). The white color of the ovaries contrasts sharply with the pink color of the encircling fallopian tubes. Crossing the pelvic brim, the ureters, gonadal vessels, and round ligament (from posterior to anterior) are found. The right ureter is generally visible under the pelvic peritoneum as it crosses over the iliac vessels, and will vermiculate if touched. The left is generally hidden by overlying sigmoid colon and mesentery.
Steps in Procedure
Lithotomy position, empty bladder, drape perineum into sterile field
Thorough abdominal exploration
Display adnexal structures by displacing uterus upwards with cervical retractor
Excision of Ovarian Cyst
Place secondary trocars at right and left paraumbilical and right and left suprapubic sites
Elevate adnexa
Excise cyst
Close defect in ovary for hemostasis
Salpingo-Oophorectomy
Expose infundibulopelvic ligament and secure gonadal vessels
Divide peritoneal reflections
Divide uterine tube at the uterine isthmus
Laparoscopic Hysterectomy
Identify ureters
Incise peritoneum between fallopian tubes (medially) and iliac vessels (laterally)
Divide round ligaments, fallopian tubes (if ovaries are preserved), and broad ligament close to uterus
Extend peritoneal incisions anteriorly and join these in cul-de-sac to produce bladder flap
Hysterectomy may be completed vaginally or from above
Secure hemostasis and close trocar sites in usual fashion
List of Structures
Uterus
Cervix
Vagina
Posterior fornix
Fallopian (uterine) tubes
Ovaries
Round ligament
Broad ligament
Suspensory (infundibulopelvic) ligament
Ovarian ligament
Lateral cervical (cardinal) ligament
Uterosacral ligament
Bladder
Ureter
Urachus
Vesicouterine pouch (anterior cul-de-sac)
Rectouterine pouch (posterior cul-de-sac, pouch of Douglas)
Internal iliac artery
Uterine artery
Ovarian (gonadal) artery
 |
Orientation and Exposure of the Adnexal Structures (Fig. 86.1)
Technical Points
Position the patient supine with the legs in stirrups (Fig. 86.1A). Empty the urinary bladder by straight catheterization (for short procedures) or indwelling Foley catheter (for long procedures). Drape the perineum to provide access to the vagina. Manipulation of the cervix (upward pressure using a cervical retractor) will displace the pelvic viscera closer to the laparoscope or to one side or the other, facilitating visualization.
Identify the round ligaments, crossing over the pelvic brim to exit through the internal inguinal rings (Fig. 86.1B). The fallopian tubes are generally somewhat pinker than the round ligaments and lie beneath them. Note the ureters crossing medially over the iliac vessels and then passing obliquely under the ovarian vessels. When gently touched with a probe or closed grasper, the ureter will vermiculate under the peritoneum and can thus be positively identified.
To display the adnexal structures (ovary and fallopian tube) on one side and create a larger working space, use the cervical retractor to displace the uterus up out of the pelvis and over to the contralateral side. Alternatively, a probe passed gently under the uterus or adnexa can provide some exposure, generally of one adnexa at a time (Fig. 86.1C, D). Ovary and fallopian tubes lie between the round and infundibulopelvic ligaments.
Anatomic Points
The pelvic sidewall triangle (Fig. 86.1C) consists of the round ligament, the infundibulopelvic ligament, and the external iliac artery. The ureter enters the pelvis medial to this triangle. The right ureter is often visible under the peritoneum overlying the external iliac artery; the left ureter is frequently obscured by the overlying sigmoid colon or its mesentery.
Laparoscopic Tubal Ligation (Fig. 86.2)
Technical Points
Identify the fallopian tubes. Elevate one with an atraumatic grasper. Numerous techniques for tubal ligation exist, none perfect. The simplest method uses a clip to occlude and gradually cut through the tubes. Place the clip on the tube and lock it closed. Repeat this on the other side.
Anatomic Points
As previously mentioned, it is imperative to differentiate round ligament from fallopian tubes. The round ligaments extend beyond the pelvic brim to the region of the internal inguinal ring. In contrast, the pinker fallopian tubes are initially less visible and terminate in the fimbriated regions, which are in close proximity to the ovaries.
Excision of Ovarian Cyst (Fig. 86.3)
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


